

Artificial intelligence algorithm for predicting cardiac arrest using electrocardiography
- PMID: 33023615
- PMCID: PMC7541213
- DOI: 10.1186/s13049-020-00791-0
Artificial intelligence algorithm for predicting cardiac arrest using electrocardiography
Abstract
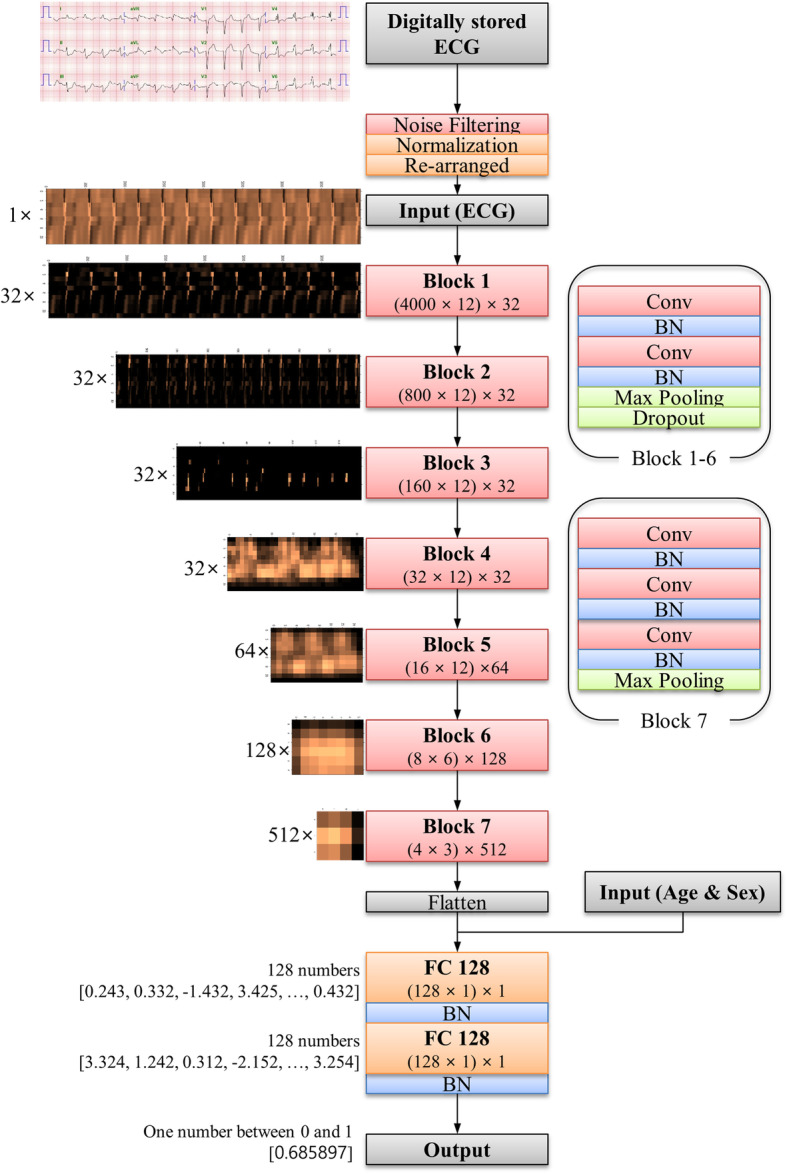
Background: In-hospital cardiac arrest is a major burden in health care. Although several track-and-trigger systems are used to predict cardiac arrest, they often have unsatisfactory performances. We hypothesized that a deep-learning-based artificial intelligence algorithm (DLA) could effectively predict cardiac arrest using electrocardiography (ECG). We developed and validated a DLA for predicting cardiac arrest using ECG.
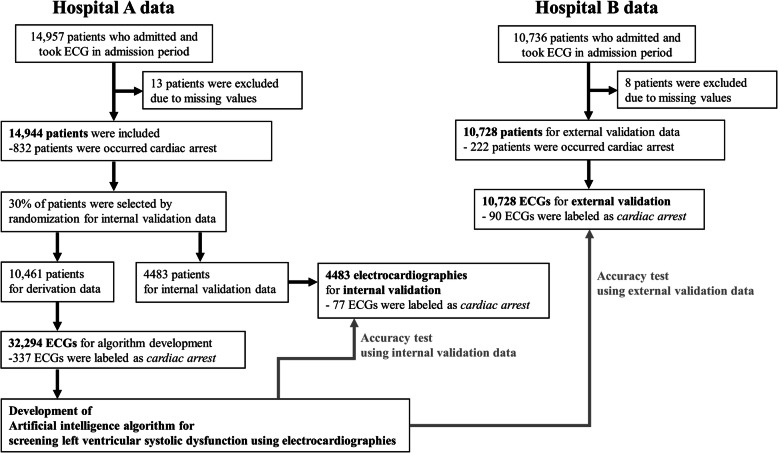
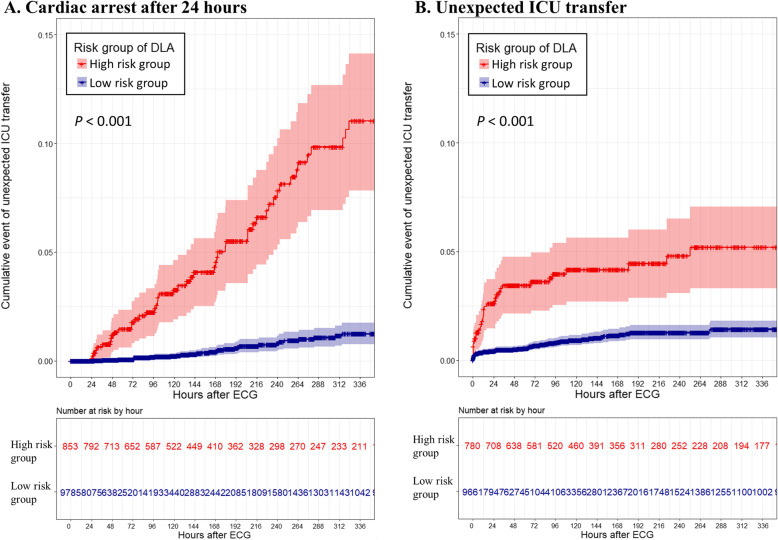
Methods: We conducted a retrospective study that included 47,505 ECGs of 25,672 adult patients admitted to two hospitals, who underwent at least one ECG from October 2016 to September 2019. The endpoint was occurrence of cardiac arrest within 24 h from ECG. Using subgroup analyses in patients who were initially classified as non-event, we confirmed the delayed occurrence of cardiac arrest and unexpected intensive care unit transfer over 14 days.
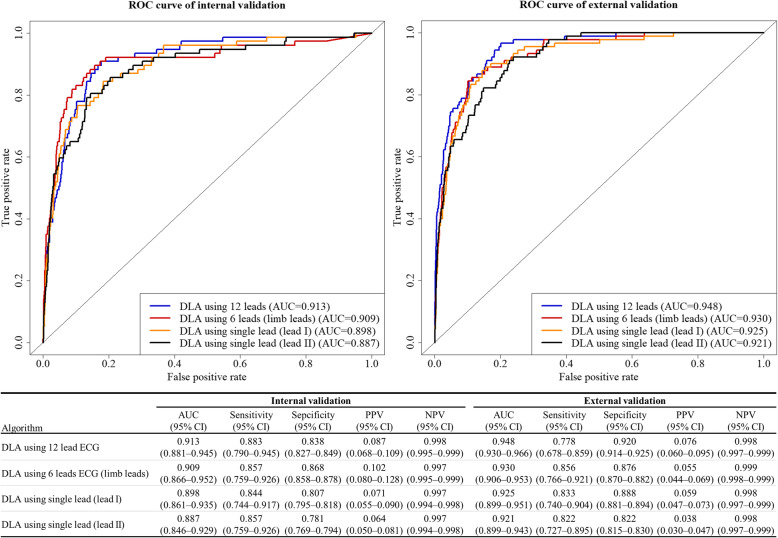
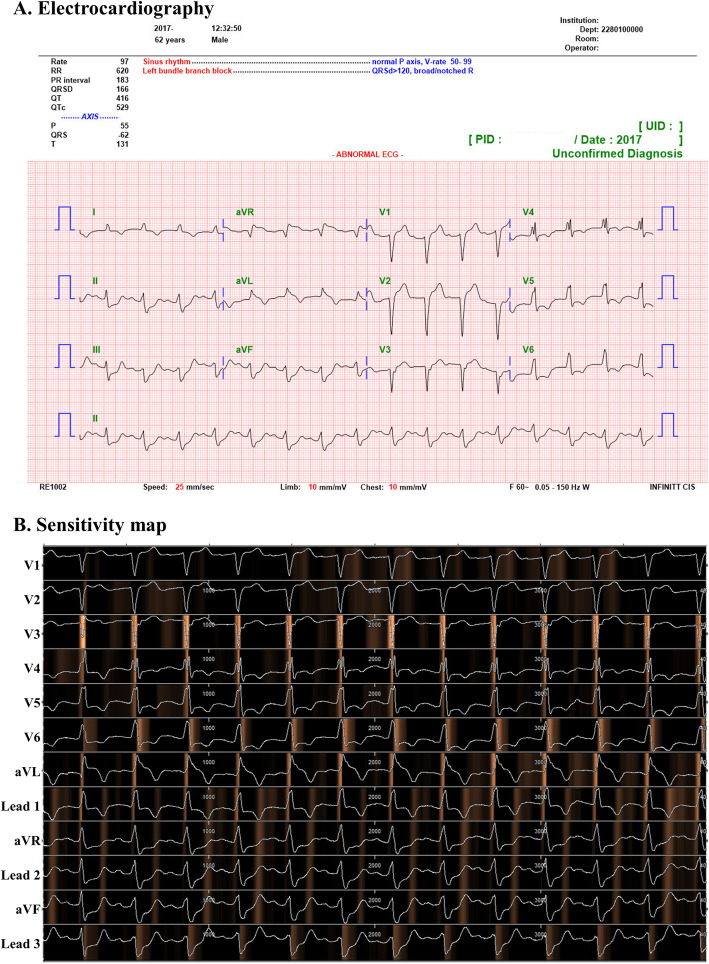
Results: We used 32,294 ECGs of 10,461 patients and 4483 ECGs of 4483 patients from a hospital were used as development and internal validation data, respectively. Additionally, 10,728 ECGs of 10,728 patients from another hospital were used as external validation data, which confirmed the robustness of the developed DLA. During internal and external validation, the areas under the receiver operating characteristic curves of the DLA in predicting cardiac arrest within 24 h were 0.913 and 0.948, respectively. The high risk group of the DLA showed a significantly higher hazard for delayed cardiac arrest (5.74% vs. 0.33%, P < 0.001) and unexpected intensive care unit transfer (4.23% vs. 0.82%, P < 0.001). A sensitivity map of the DLA displayed the ECG regions used to predict cardiac arrest, with the DLA focused most on the QRS complex.
Conclusions: Our DLA successfully predicted cardiac arrest using diverse formats of ECG. The results indicate that cardiac arrest could be screened and predicted not only with a conventional 12-lead ECG, but also with a single-lead ECG using a wearable device that employs our DLA.
Keywords: Artificial intelligence; Deep learning; Electrocardiography; Heart arrest; Hospital rapid response team.
Conflict of interest statement
KHK, KHJ, SYL, and BHO declare that they have no competing interests. JK and JP are co-founder and stakeholder in Medical AI Co Ltd., a medical artificial intelligence company. JK is researcher of Body friend co. There are no products in development or marketed products to declare. This dose not alter our adherence to Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine.
Figures
Similar articles
-
A deep learning algorithm to detect anaemia with ECGs: a retrospective, multicentre study.Lancet Digit Health. 2020 Jul;2(7):e358-e367. doi: 10.1016/S2589-7500(20)30108-4. Epub 2020 Jun 23. Lancet Digit Health. 2020. PMID: 33328095
-
Artificial intelligence algorithm for detecting myocardial infarction using six-lead electrocardiography.Sci Rep. 2020 Nov 24;10(1):20495. doi: 10.1038/s41598-020-77599-6. Sci Rep. 2020. PMID: 33235279 Free PMC article.
-
Artificial intelligence for detecting mitral regurgitation using electrocardiography.J Electrocardiol. 2020 Mar-Apr;59:151-157. doi: 10.1016/j.jelectrocard.2020.02.008. Epub 2020 Feb 27. J Electrocardiol. 2020. PMID: 32146201
-
The application of deep learning in electrocardiogram: Where we came from and where we should go?Int J Cardiol. 2021 Aug 15;337:71-78. doi: 10.1016/j.ijcard.2021.05.017. Epub 2021 May 14. Int J Cardiol. 2021. PMID: 34000355 Review.
-
Can artificial intelligence lower the global sudden cardiac death rate? A narrative review.J Electrocardiol. 2025 Mar-Apr;89:153882. doi: 10.1016/j.jelectrocard.2025.153882. Epub 2025 Jan 22. J Electrocardiol. 2025. PMID: 39862597 Review.
Cited by
-
Developing Graph Convolutional Networks and Mutual Information for Arrhythmic Diagnosis Based on Multichannel ECG Signals.Int J Environ Res Public Health. 2022 Aug 28;19(17):10707. doi: 10.3390/ijerph191710707. Int J Environ Res Public Health. 2022. PMID: 36078423 Free PMC article.
-
State-of-the-Art Deep Learning Methods on Electrocardiogram Data: Systematic Review.JMIR Med Inform. 2022 Aug 15;10(8):e38454. doi: 10.2196/38454. JMIR Med Inform. 2022. PMID: 35969441 Free PMC article. Review.
-
Enhancing Comprehensive Assessments in Chronic Heart Failure Caused by Ischemic Heart Disease: The Diagnostic Utility of Holter ECG Parameters.Medicina (Kaunas). 2024 Aug 14;60(8):1315. doi: 10.3390/medicina60081315. Medicina (Kaunas). 2024. PMID: 39202596 Free PMC article.
-
The Aspects of Running Artificial Intelligence in Emergency Care; a Scoping Review.Arch Acad Emerg Med. 2023 May 11;11(1):e38. doi: 10.22037/aaem.v11i1.1974. eCollection 2023. Arch Acad Emerg Med. 2023. PMID: 37215232 Free PMC article.
-
Sudden cardiac arrest prediction via deep learning electrocardiogram analysis.Eur Heart J Digit Health. 2025 Feb 25;6(2):170-179. doi: 10.1093/ehjdh/ztae088. eCollection 2025 Mar. Eur Heart J Digit Health. 2025. PMID: 40110219 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
