

Awake prone positioning does not reduce the risk of intubation in COVID-19 treated with high-flow nasal oxygen therapy: a multicenter, adjusted cohort study
- PMID: 33023669
- PMCID: PMC7537953
- DOI: 10.1186/s13054-020-03314-6
Awake prone positioning does not reduce the risk of intubation in COVID-19 treated with high-flow nasal oxygen therapy: a multicenter, adjusted cohort study
Abstract
Background: Awake prone positioning (awake-PP) in non-intubated coronavirus disease 2019 (COVID-19) patients could avoid endotracheal intubation, reduce the use of critical care resources, and improve survival. We aimed to examine whether the combination of high-flow nasal oxygen therapy (HFNO) with awake-PP prevents the need for intubation when compared to HFNO alone.
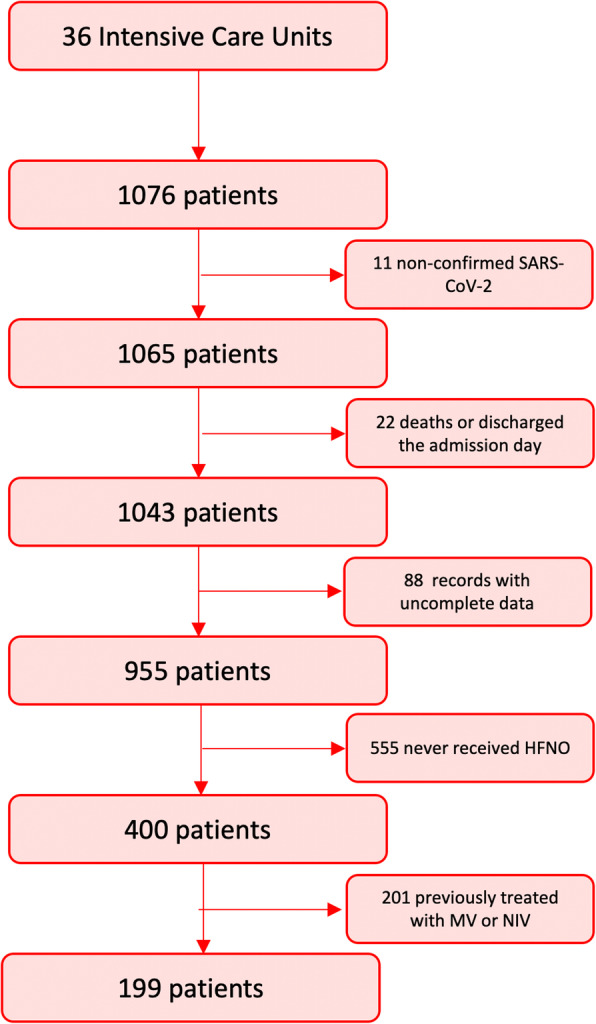
Methods: Prospective, multicenter, adjusted observational cohort study in consecutive COVID-19 patients with acute respiratory failure (ARF) receiving respiratory support with HFNO from 12 March to 9 June 2020. Patients were classified as HFNO with or without awake-PP. Logistic models were fitted to predict treatment at baseline using the following variables: age, sex, obesity, non-respiratory Sequential Organ Failure Assessment score, APACHE-II, C-reactive protein, days from symptoms onset to HFNO initiation, respiratory rate, and peripheral oxyhemoglobin saturation. We compared data on demographics, vital signs, laboratory markers, need for invasive mechanical ventilation, days to intubation, ICU length of stay, and ICU mortality between HFNO patients with and without awake-PP.
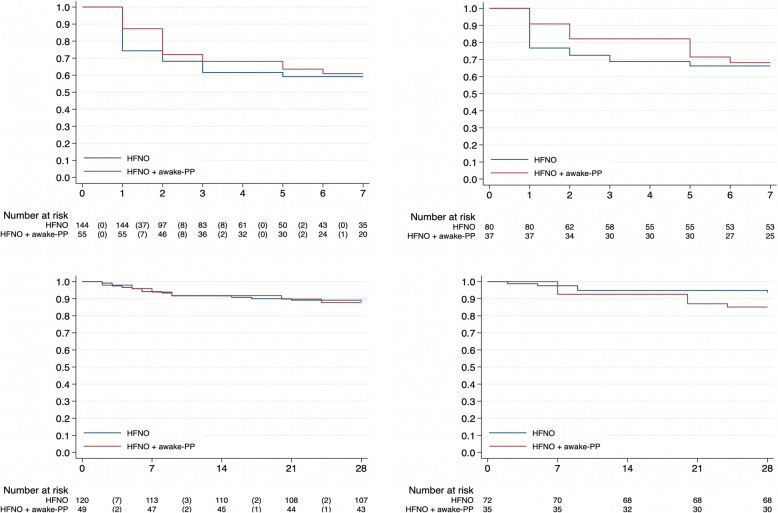
Results: A total of 1076 patients with COVID-19 ARF were admitted, of which 199 patients received HFNO and were analyzed. Fifty-five (27.6%) were pronated during HFNO; 60 (41%) and 22 (40%) patients from the HFNO and HFNO + awake-PP groups were intubated. The use of awake-PP as an adjunctive therapy to HFNO did not reduce the risk of intubation [RR 0.87 (95% CI 0.53-1.43), p = 0.60]. Patients treated with HFNO + awake-PP showed a trend for delay in intubation compared to HFNO alone [median 1 (interquartile range, IQR 1.0-2.5) vs 2 IQR 1.0-3.0] days (p = 0.055), but awake-PP did not affect 28-day mortality [RR 1.04 (95% CI 0.40-2.72), p = 0.92].
Conclusion: In patients with COVID-19 ARF treated with HFNO, the use of awake-PP did not reduce the need for intubation or affect mortality.
Keywords: Acute respiratory failure; COVID-19; Critical care; High-flow nasal oxygen therapy; Mechanical ventilation; Prone positioning.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ferrando C, Mellado-Artigas R, Gea A, et al. Patient characteristics, clinical course and factors associated to ICU mortality in critically ill patients infected with SARS-CoV-2 in Spain: a prospective, cohort, multicentre study. Rev Esp Anestesiol Reanim 2020 [Epub ahead of print]. doi: 10.1016/j.redare.2020.07.001. - PMC - PubMed
-
- https://www.formacionsanitaria.eu/documentos/Recomendations_WeVent.pdf. Last Access on 23/06/2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
