

Sex differences in cardiometabolic risk factors, pharmacological treatment and risk factor control in type 2 diabetes: findings from the Dutch Diabetes Pearl cohort
- PMID: 33023896
- PMCID: PMC7539590
- DOI: 10.1136/bmjdrc-2020-001365
Sex differences in cardiometabolic risk factors, pharmacological treatment and risk factor control in type 2 diabetes: findings from the Dutch Diabetes Pearl cohort
Abstract
Introduction: Sex differences in cardiometabolic risk factors and their management in type 2 diabetes (T2D) have not been fully identified. Therefore, we aimed to examine differences in cardiometabolic risk factor levels, pharmacological treatment and achievement of risk factor control between women and men with T2D.
Research design and methods: Cross-sectional data from the Dutch Diabetes Pearl cohort were used (n=6637, 40% women). Linear and Poisson regression analyses were used to examine sex differences in cardiometabolic risk factor levels, treatment, and control.
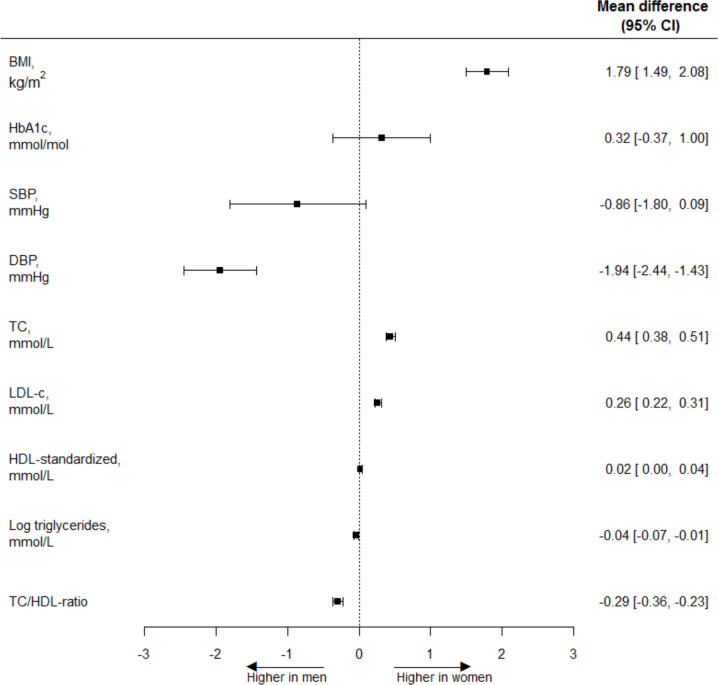
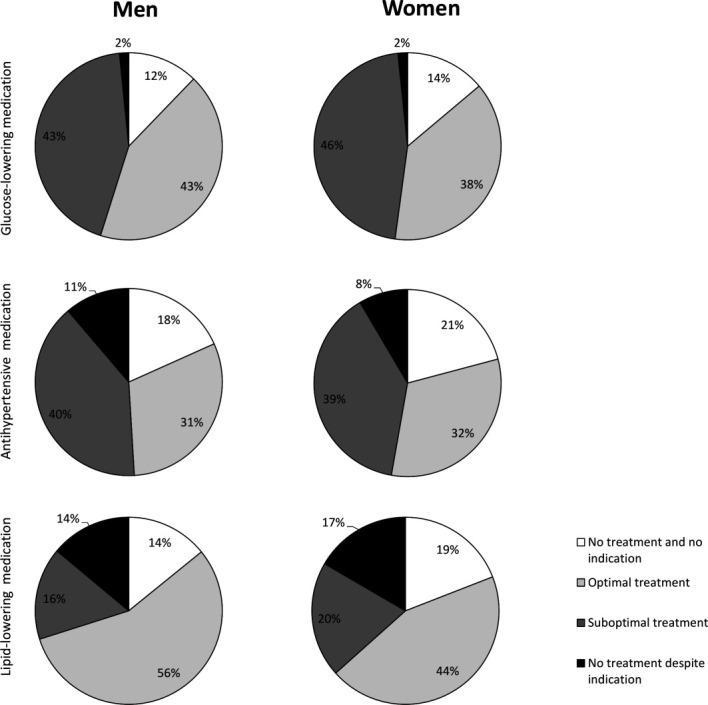
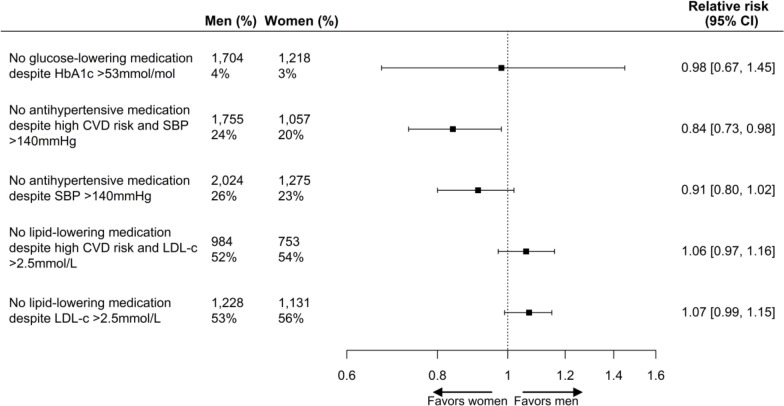
Results: Compared with men, women had a significantly higher body mass index (BMI) (mean difference 1.79 kg/m2 (95% CI 1.49 to 2.08)), while no differences were found in hemoglobin A1c (HbA1c) and systolic blood pressure (SBP). Women had lower diastolic blood pressure (-1.94 mm Hg (95% CI -2.44 to -1.43)), higher total cholesterol (TC) (0.44 mmol/L (95% CI 0.38 to 0.51)), low-density lipoprotein cholesterol (LDL-c) (0.26 mmol/L (95% CI 0.22 to 0.31)), and high-density lipoprotein cholesterol (HDL-c) sex-standardized (0.02 mmol/L (95% CI 0.00 to 0.04)), and lower TC:HDL ratio (-0.29 (95% CI -0.36 to -0.23)) and triglycerides (geometric mean ratio 0.91 (95% CI 0.85 to 0.98)). Women had a 16% higher probability of being treated with antihypertensive medication in the presence of high cardiovascular disease (CVD) risk and elevated SBP than men (relative risk 0.84 (95% CI 0.73 to 0.98)), whereas no sex differences were found for glucose-lowering medication and lipid-modifying medication. Among those treated, women were less likely to achieve treatment targets of HbA1c (0.92 (95% CI 0.87 to 0.98)) and LDL-c (0.89 (95% CI 0.85 to 0.92)) than men, while no differences for SBP were found.
Conclusions: In this Dutch T2D population, women had a slightly different cardiometabolic risk profile compared with men and a substantially higher BMI. Women had a higher probability of being treated with antihypertensive medication in the presence of high CVD risk and elevated SBP than men, and were less likely than men to achieve treatment targets for HbA1c and LDL levels.
Keywords: diabetes mellitus; epidemiology; healthcare disparities; type 2.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Kappert K, Böhm M, Schmieder R, et al. . Impact of sex on cardiovascular outcome in patients at high cardiovascular risk: analysis of the telmisartan randomized assessment study in ACE-Intolerant subjects with cardiovascular disease (TRANSCEND) and the ongoing telmisartan alone and in combination with ramipril global end point trial (ONTARGET). Circulation 2012;126:934–41. 10.1161/CIRCULATIONAHA.111.086660 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous