

Assessment of and Interventions for Women at High Risk for Breast or Ovarian Cancer: A Survey of Primary Care Physicians
- PMID: 33023915
- PMCID: PMC8021601
- DOI: 10.1158/1940-6207.CAPR-20-0407
Assessment of and Interventions for Women at High Risk for Breast or Ovarian Cancer: A Survey of Primary Care Physicians
Abstract
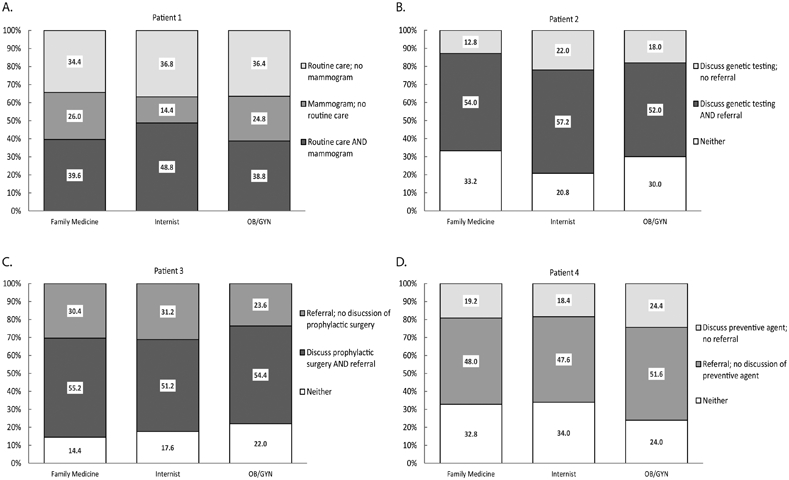
As clinical guidelines for cancer prevention refer individuals to primary care physicians (PCP) for risk assessment and clinical management, PCPs may be expected to play an increasing role in cancer prevention. It is crucial that PCPs are adequately supported to assess an individual's cancer risk and make appropriate recommendations. The objective of this study is to assess use, familiarity, attitude, and behaviors of PCPs regarding breast and ovarian cancer risk and prevention, to better understand the factors that influence their prescribing behaviors. We conducted a cross-sectional, web-based survey of PCPs in the United States, recruited from an opt-in healthcare provider panel. Invitations were sent in batches until the target sample size of 750 respondents (250 each for obstetrics/gynecology, internal medicine, and family medicine) was met. Self-reported use of breast/ovarian cancer risk assessments was low (34.7%-59.2%) compared with discussion of cancer family history (96.9%), breast exams (87.1%), and mammograms (92.8%). Although most respondents (48.0%-66.8%) were familiar with cancer prevention interventions, respondents who reported to be less familiar were more likely to report cautious attitudes. When presented with hypothetical cases depicting patients at different breast/ovarian cancer risks, up to 34.0% of respondents did not select any of the clinically recommended course(s) of action. This survey suggests that PCP use of breast/ovarian cancer risk assessment tools and ability to translate the perceived risks to clinical actions is variable. Improving implementation of cancer risk assessment and clinical management guidelines within primary care may be necessary to improve the appropriate prescribing of cancer prevention interventions.Prevention Relevance: Primary care physicians are becoming more involved in cancer prevention management, so it is important that cancer risk assessment and medical society guideline recommendations for cancer prevention are better integrated into primary care to improve appropriate prescribing of cancer prevention interventions and help reduce cancer risk.
©2020 American Association for Cancer Research.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
Similar articles
-
Cancer Prevention in Primary Care: Perception of Importance, Recognition of Risk Factors and Prescribing Behaviors.Am J Med. 2020 Jun;133(6):723-732. doi: 10.1016/j.amjmed.2019.11.017. Epub 2019 Dec 17. Am J Med. 2020. PMID: 31862335 Free PMC article.
-
Primary care physicians' familiarity, beliefs, and perceived barriers to practice guidelines in non-diabetic CKD: a survey study.BMC Nephrol. 2014 Apr 22;15:64. doi: 10.1186/1471-2369-15-64. BMC Nephrol. 2014. PMID: 24755164 Free PMC article.
-
Physician Breast Cancer Screening Recommendations Following Guideline Changes: Results of a National Survey.JAMA Intern Med. 2017 Jun 1;177(6):877-878. doi: 10.1001/jamainternmed.2017.0453. JAMA Intern Med. 2017. PMID: 28395005 Free PMC article. No abstract available.
-
Are we ready for the challenge of implementing risk-based breast cancer screening and primary prevention?Breast. 2018 Jun;39:24-32. doi: 10.1016/j.breast.2018.02.029. Epub 2018 Mar 10. Breast. 2018. PMID: 29529454 Review.
-
Mathematical models of breast and ovarian cancers.Wiley Interdiscip Rev Syst Biol Med. 2016 Jul;8(4):337-62. doi: 10.1002/wsbm.1343. Epub 2016 Jun 3. Wiley Interdiscip Rev Syst Biol Med. 2016. PMID: 27259061 Free PMC article. Review.
Cited by
-
Validation study of risk-reduction activities after personalized breast cancer education tool in the WISDOM study.NPJ Breast Cancer. 2024 Oct 14;10(1):90. doi: 10.1038/s41523-024-00681-z. NPJ Breast Cancer. 2024. PMID: 39397069 Free PMC article.
-
Validation Study on Risk-Reduction Activities after Exposure to a Personalized Breast Cancer Risk-Assessment Education Tool in High-Risk Women in the WISDOM Study.Res Sq [Preprint]. 2023 May 10:rs.3.rs-2787493. doi: 10.21203/rs.3.rs-2787493/v1. Res Sq. 2023. Update in: NPJ Breast Cancer. 2024 Oct 14;10(1):90. doi: 10.1038/s41523-024-00681-z. PMID: 37214889 Free PMC article. Updated. Preprint.
-
Report from an NCI Roundtable: Cancer Prevention in Primary Care.Cancer Prev Res (Phila). 2022 May 3;15(5):273-278. doi: 10.1158/1940-6207.CAPR-21-0599. Cancer Prev Res (Phila). 2022. PMID: 35502552 Free PMC article.
-
Patient, Care Partner, and Physician Voices in Treatment Decision-Making for Multiple Myeloma.Patient Prefer Adherence. 2024 Oct 19;18:2147-2158. doi: 10.2147/PPA.S474722. eCollection 2024. Patient Prefer Adherence. 2024. PMID: 39445100 Free PMC article.
-
Talking numbers: how women and providers use risk scores during and after risk counseling - a qualitative investigation from the NRG Oncology/NSABP DMP-1 study.BMJ Open. 2023 Nov 19;13(11):e073138. doi: 10.1136/bmjopen-2023-073138. BMJ Open. 2023. PMID: 37984961 Free PMC article. Clinical Trial.
References
-
- Daly MB, Pilarski R, Yurgelun MB, Berry MP, Buys SS, Dickson P, et al. NCCN Guidelines Insights: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic, Version 1.2020. J Natl Compr Canc Netw. 2020;18:380–91. - PubMed
-
- Force USPST, Owens DK, Davidson KW, Krist AH, Barry MJ, Cabana M, et al. Risk Assessment, Genetic Counseling, and Genetic Testing for BRCA-Related Cancer: US Preventive Services Task Force Recommendation Statement. JAMA : the journal of the American Medical Association. 2019;322:652–65. - PubMed
-
- Bevers TB, Helvie M, Bonaccio E, Calhoun KE, Daly MB, Farrar WB, et al. Breast Cancer Screening and Diagnosis, Version 3.2018, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2018;16:1362–89. - PubMed
-
- Siu AL, Force USPST. Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2016;164:279–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
