

Junctional ectopic tachycardia (JET)
- PMID: 33024461
- PMCID: PMC7532275
- DOI: 10.1002/joa3.12410
Junctional ectopic tachycardia (JET)
Abstract
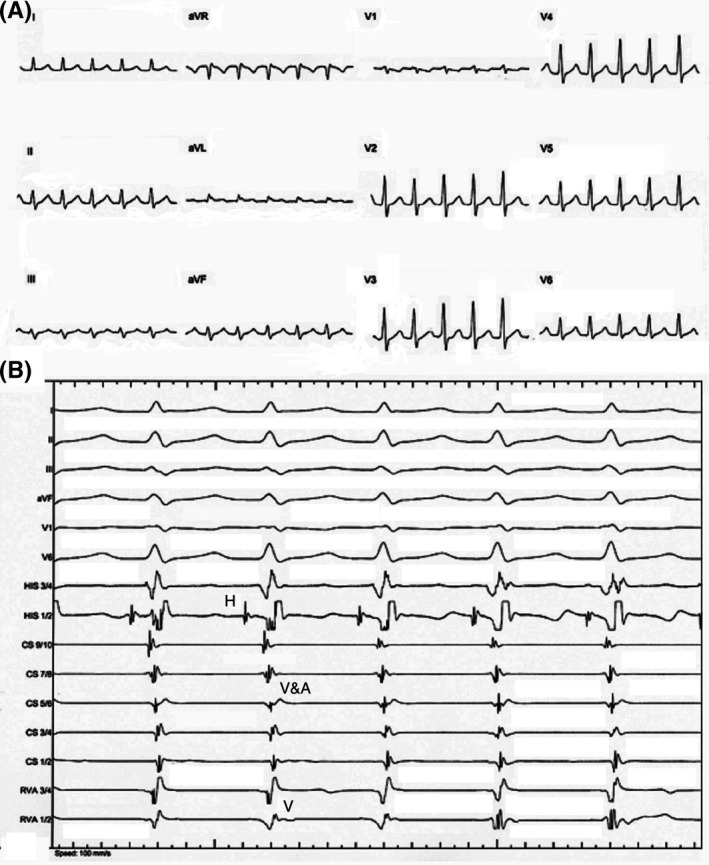
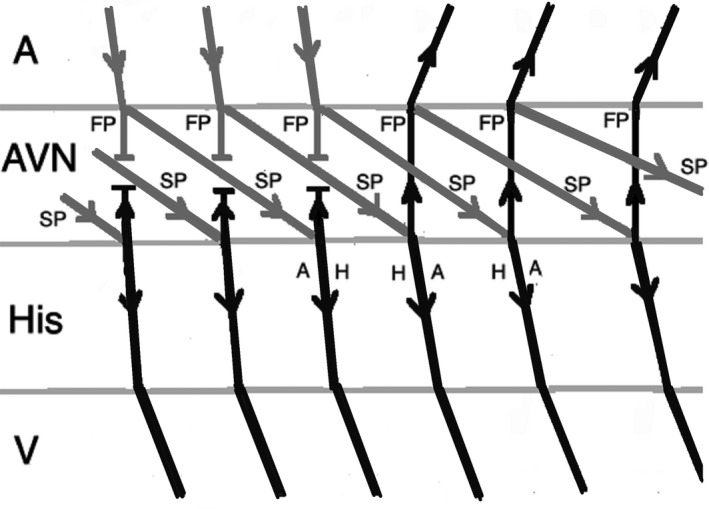
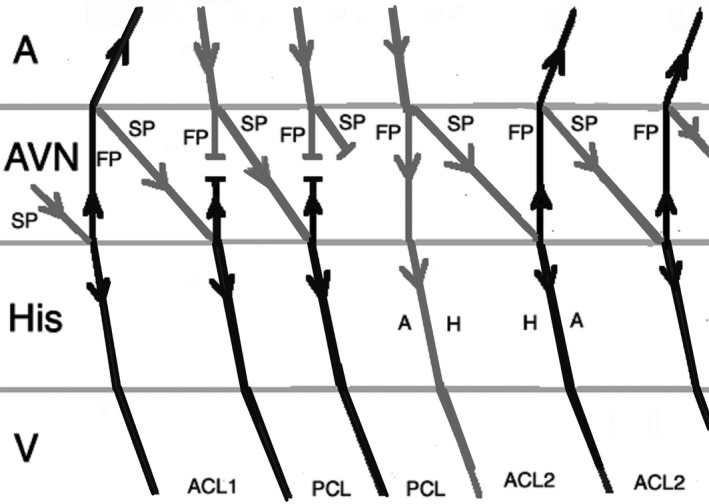
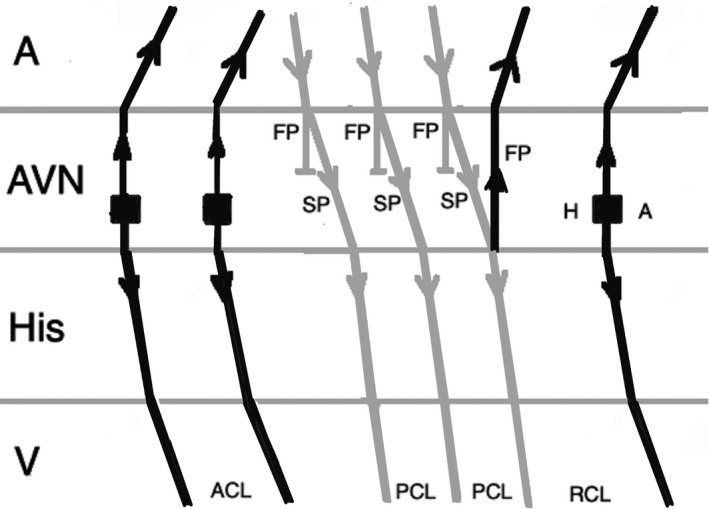
Junctional ectopic tachycardia (JET) is a tachyarrhythmia arising from the atrioventricular node and His bundle area. Enhanced normal automaticity has been postulated as the mechanism of JET in the majority of patients. It is more common in children and can be seen as congenital or in postoperative settings. It is often a narrow complex tachycardia but can present as a wide complex tachycardia as a result of aberrant conduction. Its differentiation from other arrhythmias especially atrioventricular nodal reentrant tachycardia (AVNRT) can be challenging. Medical treatment of JET is difficult, and catheter ablation remains the mainstay of treatment in refractory cases with a high risk of atrioventricular block and recurrence.
Keywords: arrhythmia; ectopic; focal; junctional tachycardia; pediatrics; postoperative.
© 2020 The Authors. Journal of Arrhythmia published by John Wiley & Sons Australia, Ltd on behalf of Japanese Heart Rhythm Society.
Conflict of interest statement
The authors declare no conflict of interests for this article.
Figures

References
-
- Liu CF, Ip JE, Markowitz SM, Lerman BB. Junctional tachycardia In: Zipes D, Jalife J, Stevenson W, editors. Cardiac electrophysiology: from cell to bedside, 7th edn Philadelphia, PA: Elsevier, 2018; p. 768–775.
-
- Gonzalez MD, Banchs JE, Moukabary T, Rivera J. Ablation of atrioventricular junctional tachycardia: atrioventricular variants and focal junctional tachycardia In: Huang SKS, Miller JM, editors. Catheter ablation of cardiac arrhythmias, 4th edn Philadelphia, PA: Elsevier, 2020; p. 316–348.
-
- Collins KK, Van Hare GF, Kertesz NJ, Law IH, Bar‐Cohen Y, Dubin AM, Etheridge SP, Berul CI, Avari JN, Tuzcu V, Sreeram N, Schaffer MS, Fournier A, Sanatani S, Snyder CS, Smith RT, Arabia L, Hamilton R, Chun T, Liberman L, Kakavand B, Paul T, Tanel RE. Pediatric non post‐operative junctional ectopic tachycardia: Medical management and interventional therapies. J Am Coll Cardiol. 2009;53(8):690–7. - PubMed
-
- Ozyilmaz EY, Ozyilmaz S, Guzeltas A. Junctional ectopic tachycardia in late period after early postoperative complete atrioventricular block: Messenger of return to normal sinus rhythm? Explanation with four case series. J Electrocardiol. 2017;50:378–382. - PubMed
-
- Pierick AR, Law IH, Muldonado JR, Bergen NH. Junctional ectopic tachycardia localization and procedural approach using cryoablation. Pacing Clin Electrophysiol. 2017;40:655–660. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
