

Defining Cardiac Dysautonomia - Different Types, Overlap Syndromes; Case-based Presentations
- PMID: 33024503
- PMCID: PMC7533131
- DOI: 10.4022/jafib.2403
Defining Cardiac Dysautonomia - Different Types, Overlap Syndromes; Case-based Presentations
Abstract
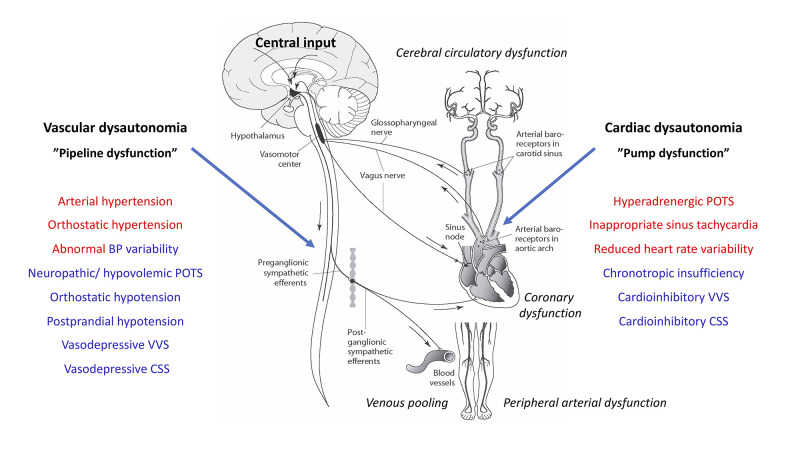
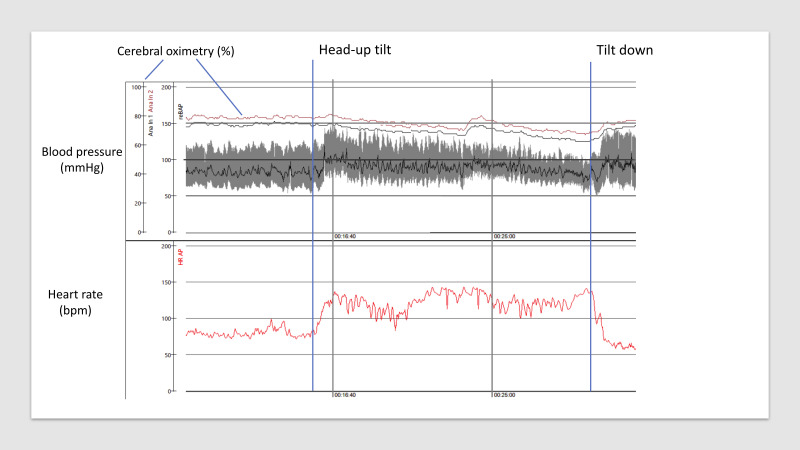
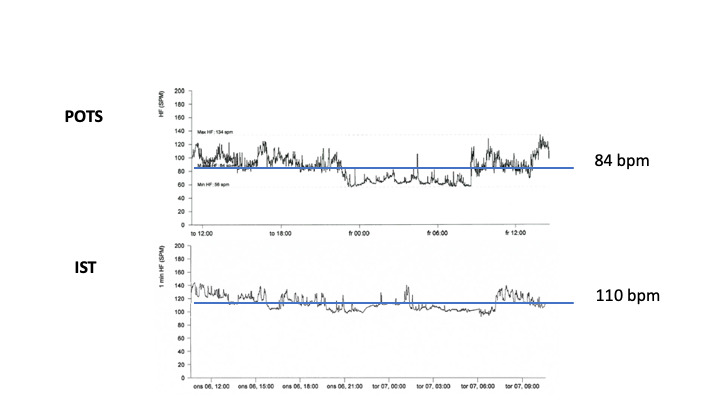
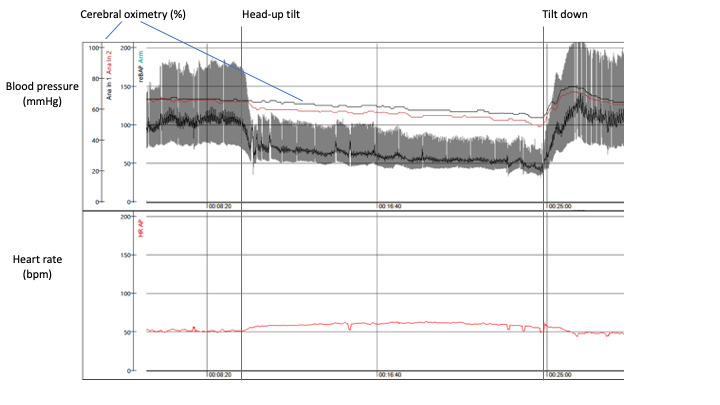
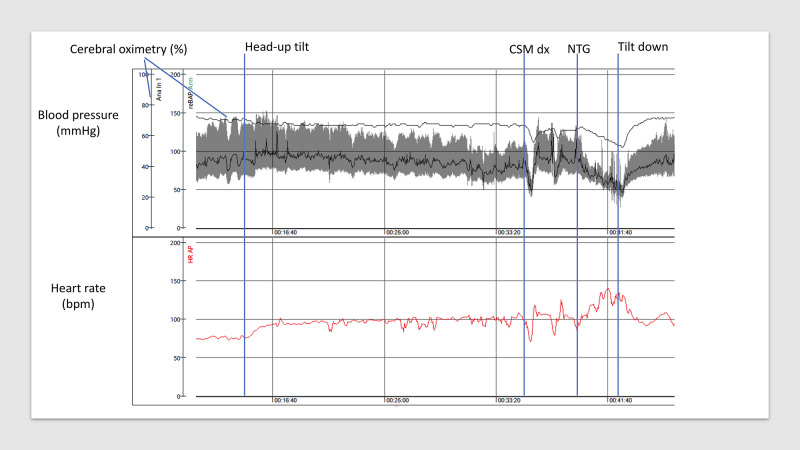
The cardiovascular branch of autonomic nervous system (ANS) is responsible for the regulation of heart rate, blood pressure, and maintaining homeostasis during physiological stress such as exercise and standing upright. ANS constantly controls the rate and force of heart contractions and the vascular tone with the aim to maintain the sufficient tissue perfusion with oxygenated blood and secure venous return to the heart. Dysautonomias, result of ANS malfunction, are often found in patients with cardiovascular symptoms. Apart from the most prevalent one, arterial hypertension, the cardiovascular dysautonomic continuum encompasses other important although less known conditions: postural orthostatic tachycardia syndrome, inappropriate sinus tachycardia, orthostatic hypotension and reflex syncope. Moreover, heart diseases may evoke autonomic imbalance by themselves; cardiac pump failure is usually associated with sympathetic hyperactivity, neuroendocrine vasopressor activation, higher heart rate, reduced heart rate variability and baroreflex hyposensitivity, all of which are predictors of adverse outcomes. Cardiologists and electrophysiologist frequently see patients for the evaluation and management of unexplained syncope, orthostatic intolerance, heart rhythm abnormalities and symptoms of palpitations. Recognizing the presence of cardiac dysautonomia is an important skill which is necessary for the appropriate evaluation and treatment of these patients. Clinical presentations may overlap, and the importance of a thorough history cannot be over-emphasized. In this review we will present a cases of a patients with cardiac dysautonomia which is illustrative of a typical patient experience, followed by a review of the autonomic nervous system and discussion of prevalence, clinical presentation, and pathophysiology of common cardiac dysautonomias.
Keywords: Atrial fibrillation; Autonomic dysfunction; Autonomic nervous system; Obesity; Risk factors.
Figures
References
-
- Novak Peter. Autonomic Disorders. Am. J. Med. 2019 Apr;132 (4):420–436. - PubMed
-
- Kaufmann Horacio, Norcliffe-Kaufmann Lucy, Palma Jose-Alberto. Baroreflex Dysfunction. N. Engl. J. Med. 2020 Jan 09;382 (2):163–178. - PubMed
-
- Cooper V L, Hainsworth R. Carotid baroreceptor reflexes in humans during orthostatic stress. Exp. Physiol. 2001 Sep;86 (5):677–81. - PubMed
-
- Novak V, Novak P, Spies J M, Low P A. Autoregulation of cerebral blood flow in orthostatic hypotension. Stroke. 1998 Jan;29 (1):104–11. - PubMed
LinkOut - more resources
Full Text Sources