

Posterior Glenoid Augmentation With Extra-articular Iliac Crest Autograft for Recurrent Posterior Shoulder Instability
- PMID: 33024660
- PMCID: PMC7528205
- DOI: 10.1016/j.eats.2020.04.023
Posterior Glenoid Augmentation With Extra-articular Iliac Crest Autograft for Recurrent Posterior Shoulder Instability
Abstract
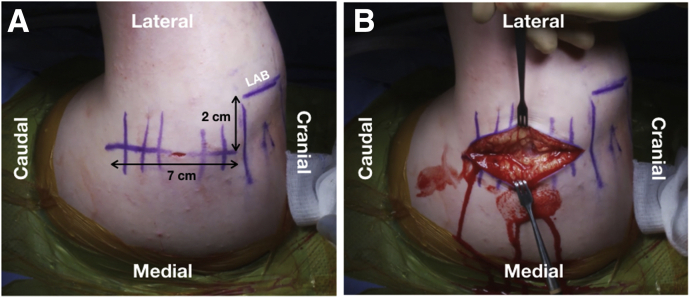
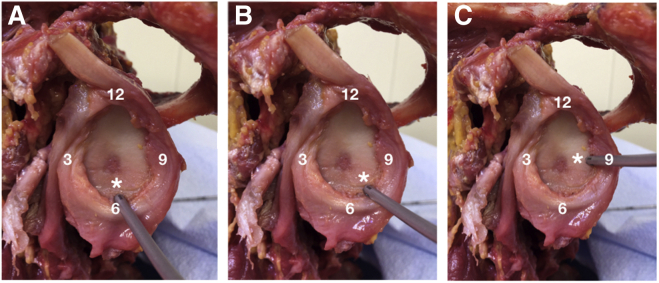
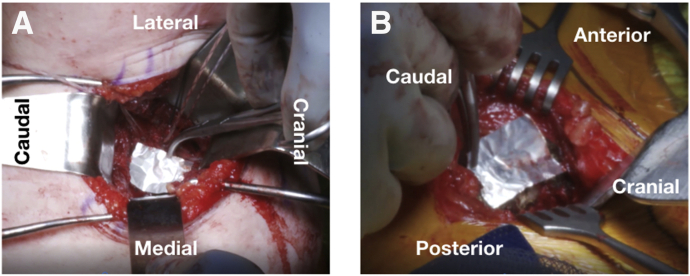
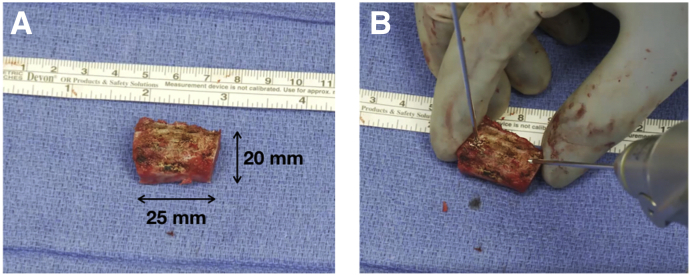
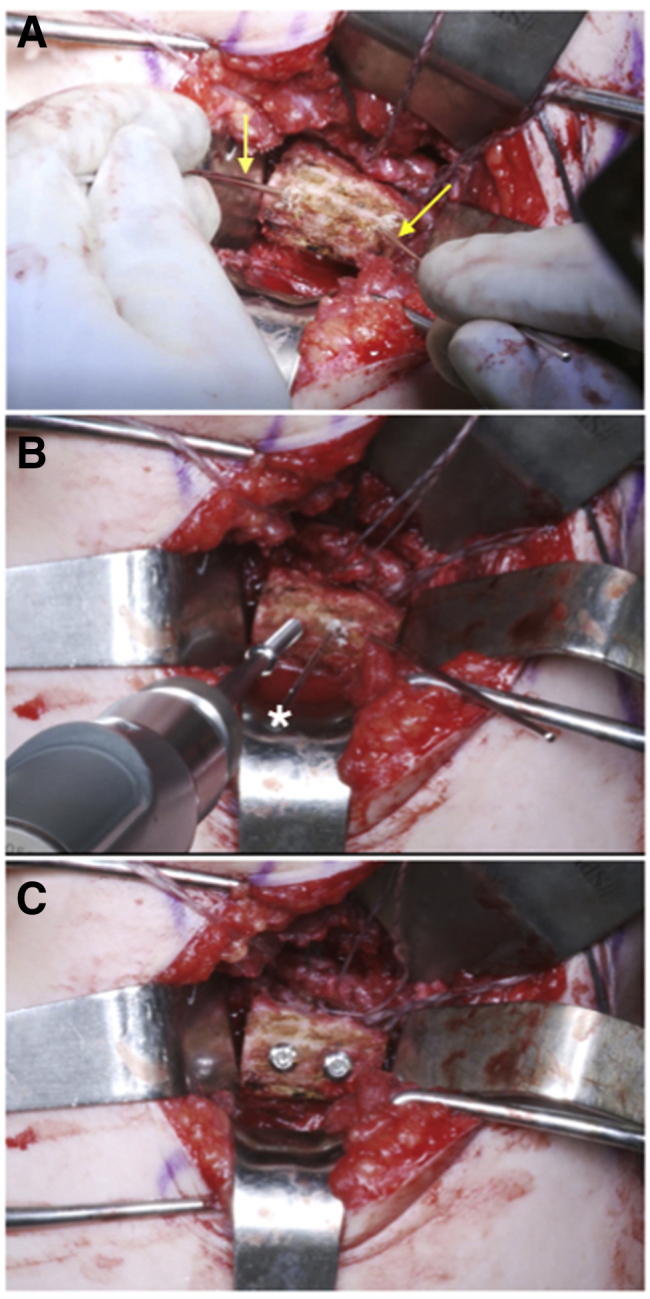
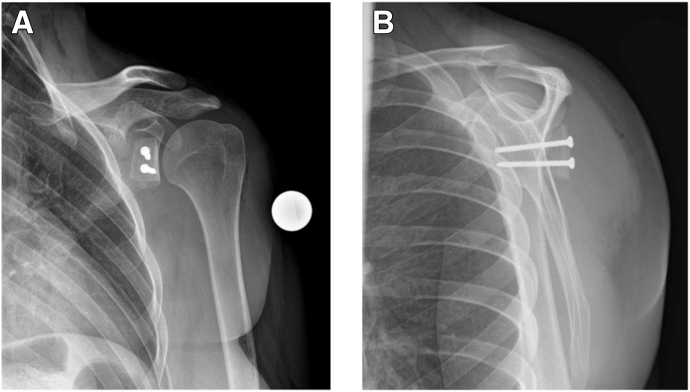
Several techniques have been described for bone block augmentation as a treatment for posterior shoulder instability, including intra-articular distal tibial allograft and extra-articular iliac crest autograft. Although indications are not yet well defined, these bone augmentation procedures are considered in patients with glenoid bone loss, increased glenoid retroversion, previous failed posterior soft-tissue repair, and insufficient posterior capsulolabral tissue. In patients with posterior glenoid bone loss, the senior author (P.J.M.) recommends intra-articular glenoid reconstruction with a fresh distal tibial osteoarticular allograft. In patients with insufficient posterior capsulolabral tissue, the senior author prefers an extra-articular iliac crest autograft to buttress the posterior soft-tissue restraints. This technique guide outlines extra-articular iliac crest autograft treatment for recurrent posterior shoulder instability in patients with insufficient posterior soft tissues due to prior failed surgery. After an open capsulolabral repair is performed using suture anchors, the bone block is placed extra-articularly on the posterior glenoid neck.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures

References
-
- Owens B.D., Duffey M.L., Nelson B.J., DeBerardino T.M., Taylor D.C., Mountcastle S.B. The incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007;35:1168–1173. - PubMed
-
- Zacchilli M.A., Owens B.D. Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am. 2010;92:542–549. - PubMed
-
- Bernhardson A.S., Murphy C.P., Aman Z.S., LaPrade R.F., Provencher M.T. A prospective analysis of patients with anterior versus posterior shoulder instability: A matched cohort examination and surgical outcome analysis of 200 patients. Am J Sports Med. 2019;47:682–687. - PubMed
-
- Arner J.W., McClincy M.P., Bradley J.P. Arthroscopic stabilization of posterior shoulder instability is successful in American football players. Arthroscopy. 2015;31:1466–1471. - PubMed
-
- Bradley J.P., Arner J.W., Jayakumar S., Vyas D. Risk factors and outcomes of revision arthroscopic posterior shoulder capsulolabral repair. Am J Sports Med. 2018;46:2457–2465. - PubMed
LinkOut - more resources
Full Text Sources
