

Management of Traumatic Coracoid Fracture and Anterior Shoulder Instability With a Modified Arthroscopic Latarjet Technique
- PMID: 33024675
- PMCID: PMC7528615
- DOI: 10.1016/j.eats.2020.05.016
Management of Traumatic Coracoid Fracture and Anterior Shoulder Instability With a Modified Arthroscopic Latarjet Technique
Abstract
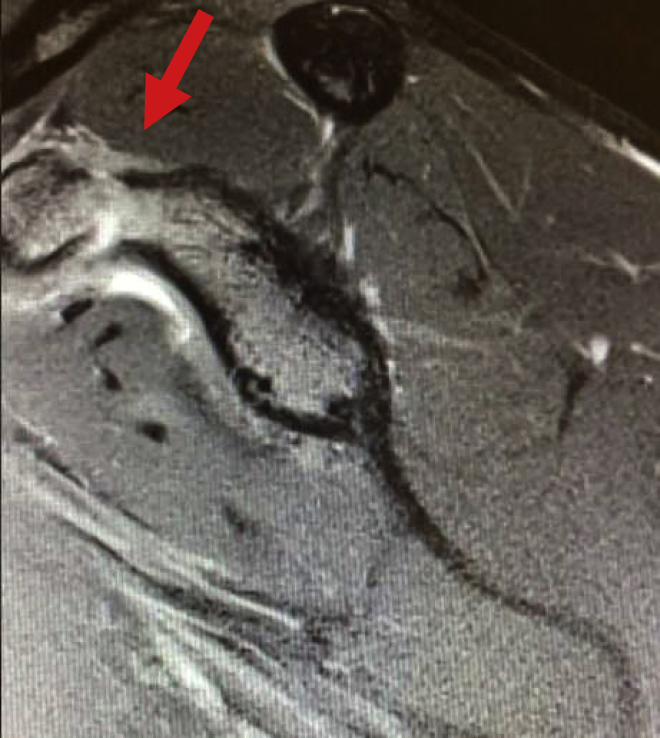
Coracoid fractures are an uncommon injury and typically occur in the setting of high-energy trauma. Isolated injury to the coracoid is rare; therefore, a high suspicion for concomitant shoulder injuries should exist. These associated injuries have been shown to be acromioclavicular dislocations, clavicular and acromial fractures, scapular spine fractures, rotator cuff tears, and anterior shoulder dislocations. Although most of these shoulder injuries respond to nonsurgical treatment, there are case reports and literature reviews that present more complicated injuries requiring surgical intervention. Shoulder dislocations with associated coracoid fractures can also manifest glenoid bone loss resulting in continued instability. In this scenario, the fractured coracoid can be used to address the glenoid bone loss, as well as the continued instability. Regarding technique, other authors have described an open procedure with screw or anchor fixation. This Technical Note describes our technique for treating a displaced Ogawa type II coracoid process fracture with concomitant anterior shoulder dislocation by an arthroscopic Latarjet procedure using the fractured coracoid.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures









References
-
- Knapik D.M., Patel S.H., Wetzel R.J., Voos J.E. Prevalence and management of coracoid fracture sustained during sporting activities and time to return to sport. Am J Sports Med. 2018;46:753–758. - PubMed
-
- Gottschalk H.P., Browne R.H., Starr A.J. Shoulder girdle: Patterns of trauma and associated injuries. J Orthop Trauma. 2011;25:266–271. - PubMed
-
- Ogawa K., Yoshida A., Takahashi M., Ui M. Fractures of the coracoid process. J Bone Joint Surg Br. 1997;79:17–19. - PubMed
-
- Ogawa K., Matsumura N., Ikegami H. Coracoid fractures: Therapeutic strategy and surgical outcomes. J Trauma Acute Care Surg. 2012;72:E20–E26. - PubMed
LinkOut - more resources
Full Text Sources
