

Latarjet Cerclage: The Metal-Free Fixation
- PMID: 33024683
- PMCID: PMC7528757
- DOI: 10.1016/j.eats.2020.05.024
Latarjet Cerclage: The Metal-Free Fixation
Abstract
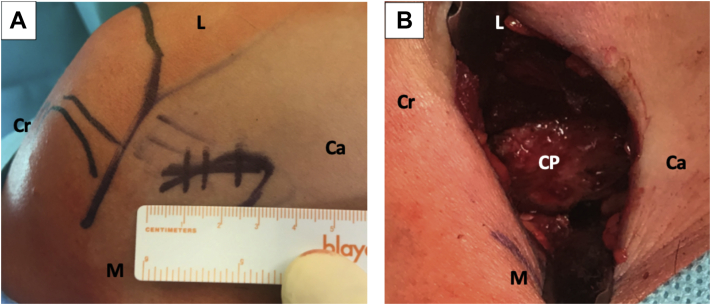
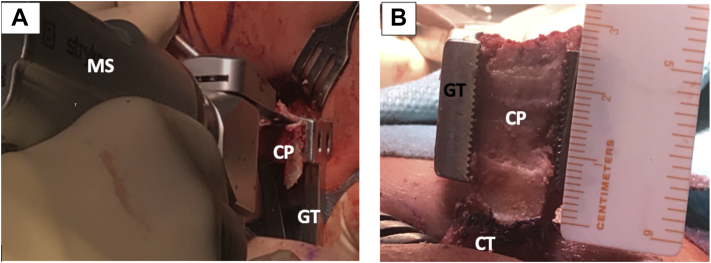
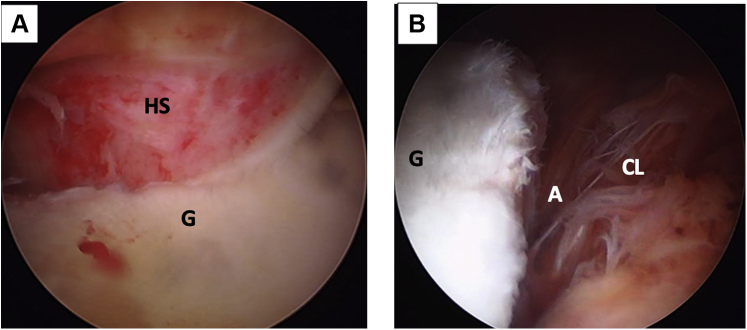
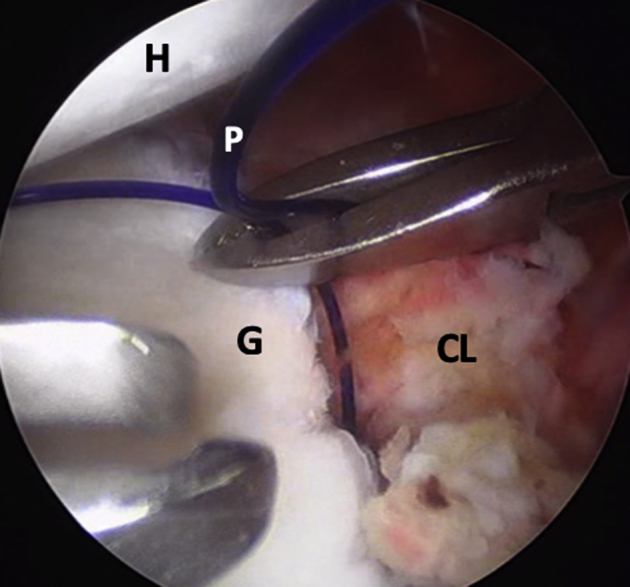
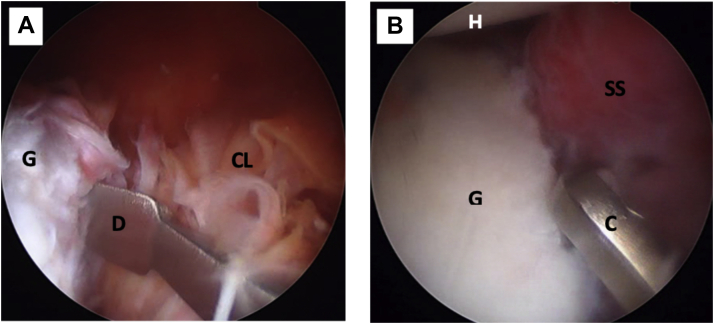
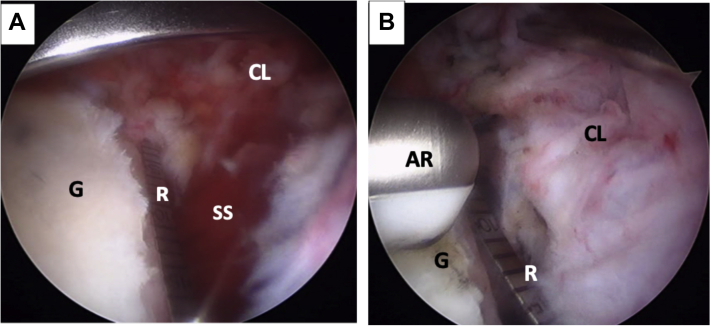
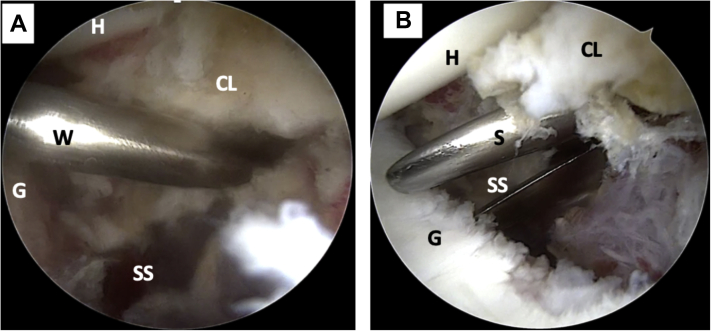
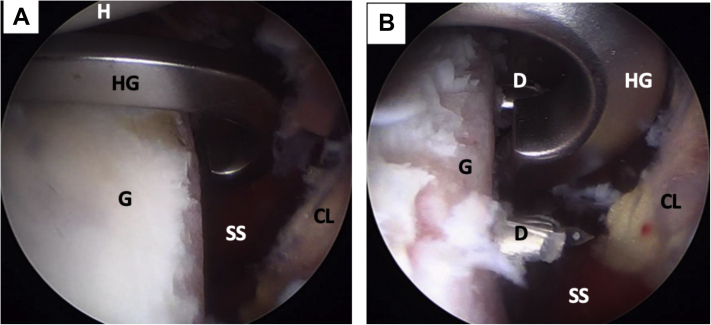
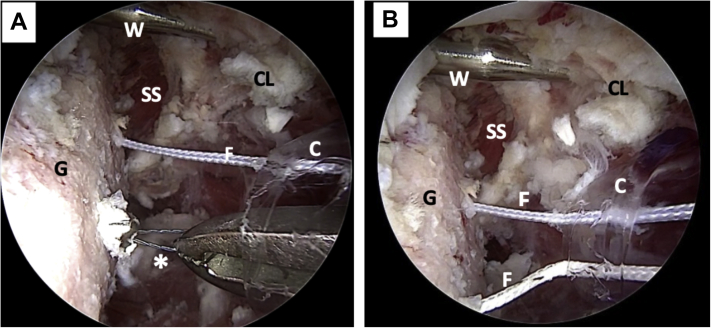
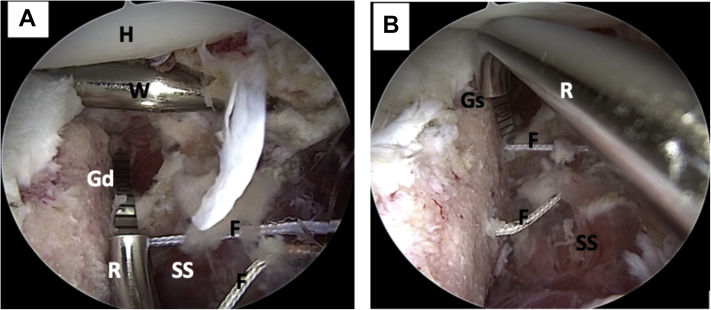
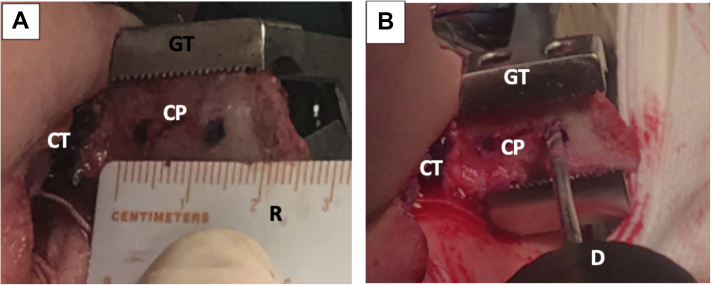
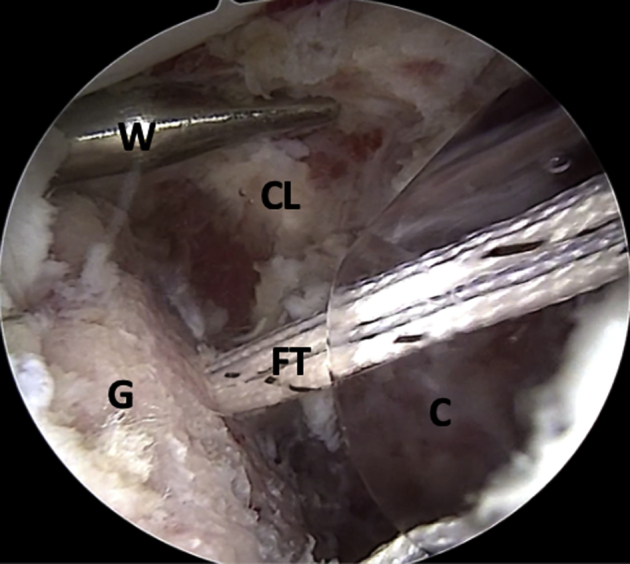
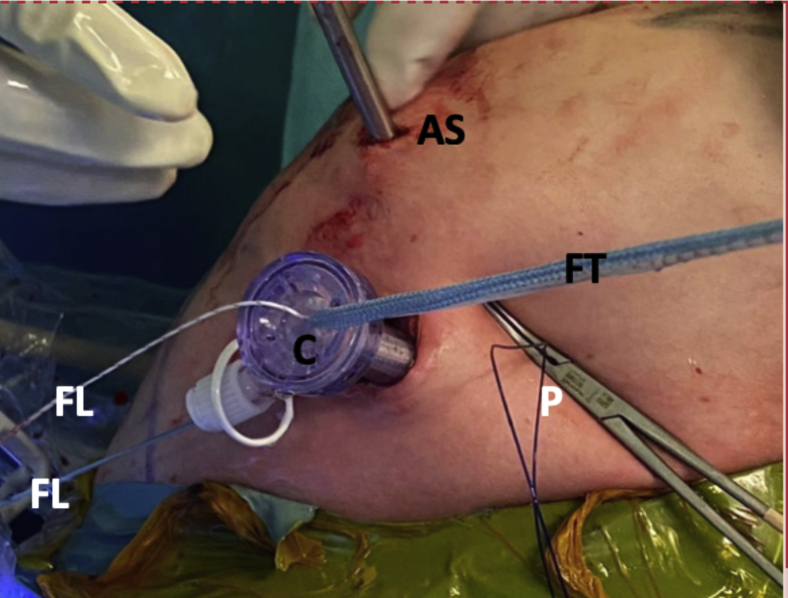
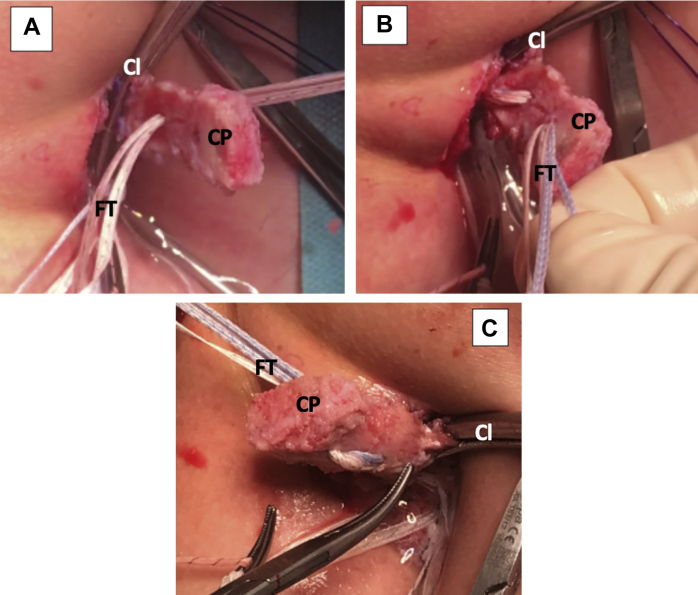
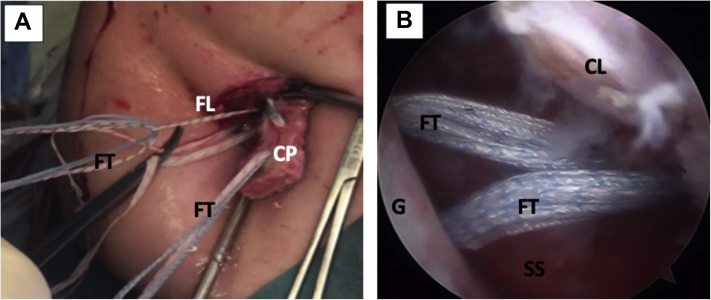
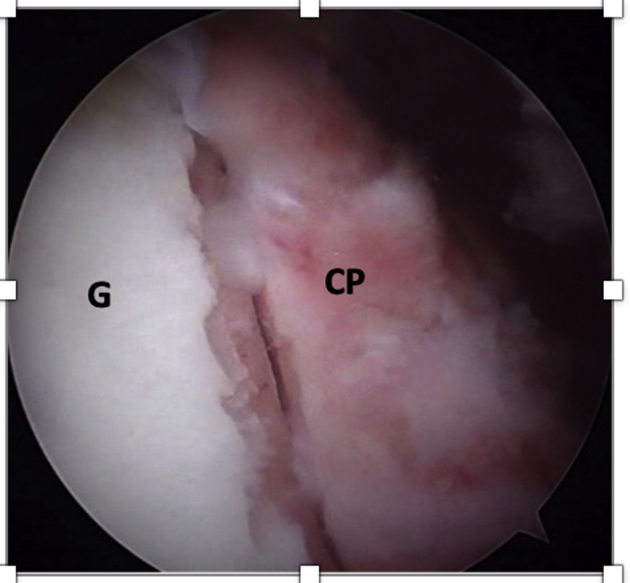
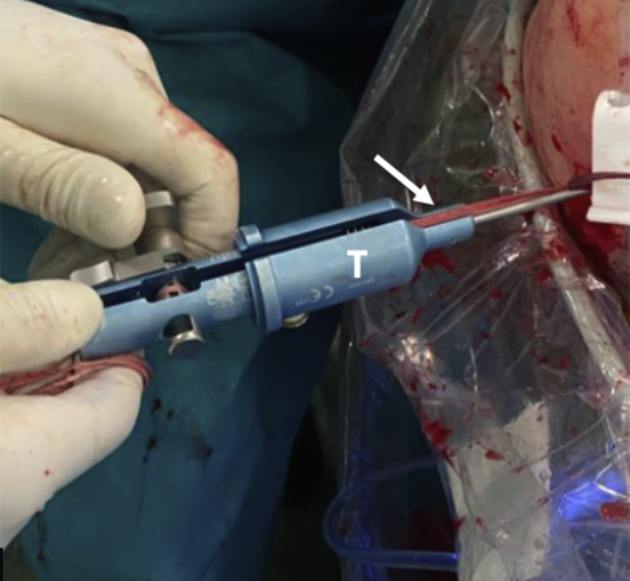
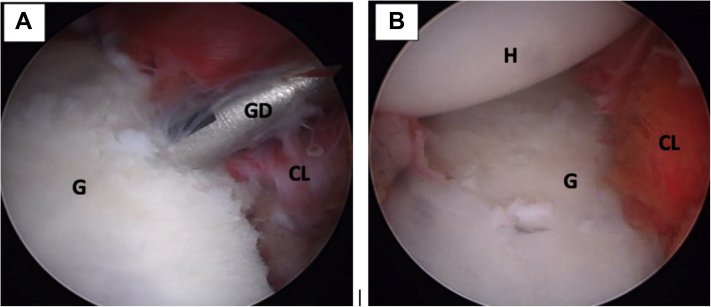
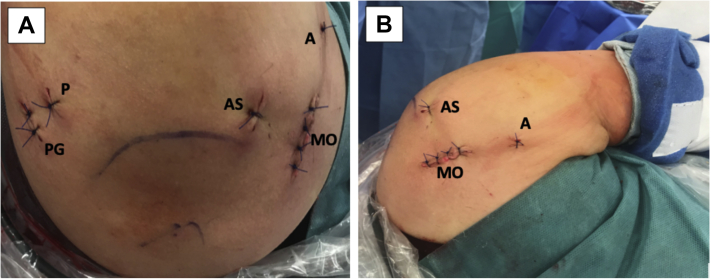
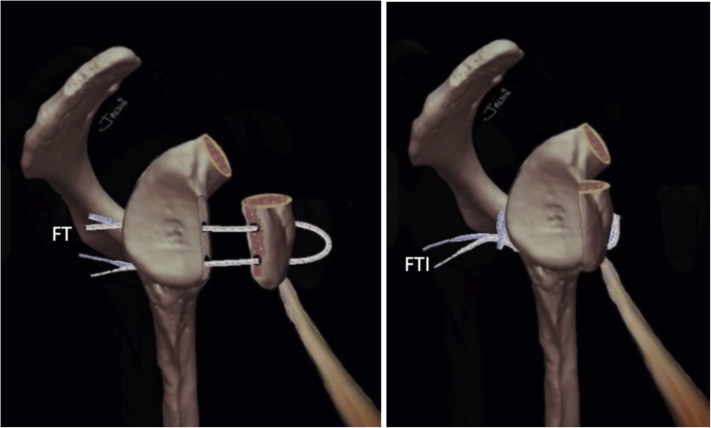
The Latarjet technique is a widely used technique for anterior shoulder instability with glenoid bone defects, irreparable capsuloligamentous lesion, or in patients at greater risk of recurrence. The use of this technique has been reported to obtain satisfactory clinical and biomechanical results. Although other methods exist, the coracoid process is typically fixed with 2 metal screws. Complications related to metal fixation are very frequently reported. In an attempt to avoid these complications, we developed this arthroscopically assisted metal-free Latarjet technique in which we fix a coracoid graft using four cerclage tapes to achieve a strong, stable fixation, thus mimicking a plate.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier.
Figures
References
-
- Latarjet M. Treatment of recurrent dislocation of the shoulder. Lyon Chir. 1954;49:994–997. - PubMed
-
- Provencher M.T., Bhatia S., Ghodadra N.S. Recurrent shoulder instability: Current concepts for evaluation and management of glenoid bone loss. J Bone Joint Surg A. 2010;92(suppl 2):133–151. - PubMed
-
- Burkhart S.S., De Beer J.F., Barth J.R.H., Criswell T., Roberts C., Richards D.P. Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss. Arthroscopy. 2007;23:1033–1041. - PubMed
-
- Butt U., Charalambous C.P. Complications associated with open coracoid transfer procedures for shoulder instability. J Shoulder Elbow Surg. 2012;21:1110–1119. - PubMed
-
- Giles J.W., Boons H.W., Elkinson I. Does the dynamic sling effect of the Latarjet procedure improve shoulder stability? A biomechanical evaluation. J Shoulder Elbow Surg. 2013;22:821–827. - PubMed
