

Primary sclerosing cholangitis and autoimmune hepatitis overlap syndrome associated with inflammatory bowel disease: A case report and systematic review
- PMID: 33024765
- PMCID: PMC7520795
- DOI: 10.12998/wjcc.v8.i18.4075
Primary sclerosing cholangitis and autoimmune hepatitis overlap syndrome associated with inflammatory bowel disease: A case report and systematic review
Abstract
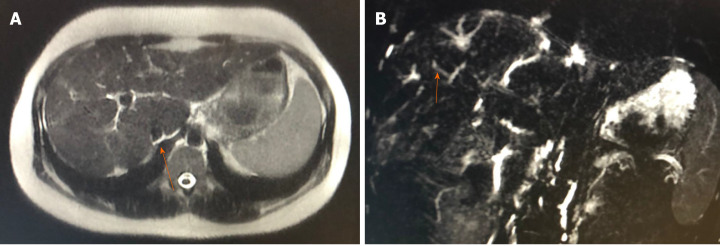
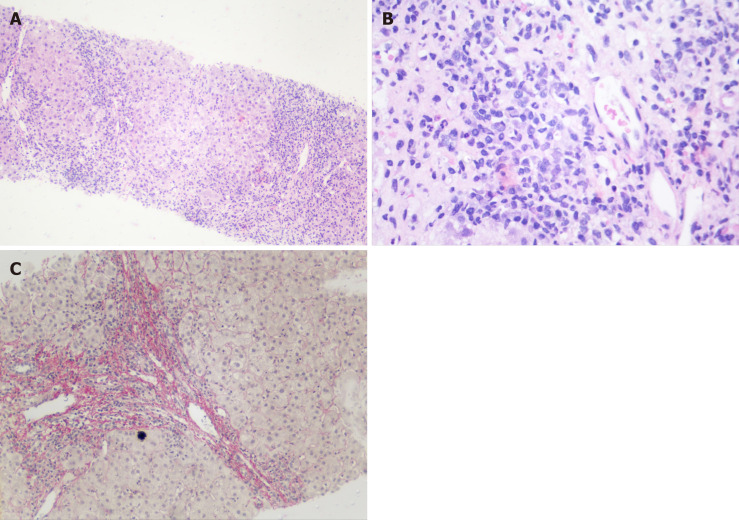
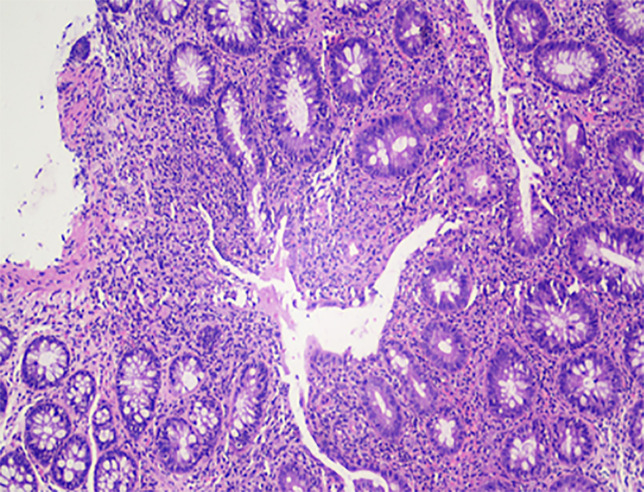
Background: A previously healthy 22-year-old woman presented with abdominal pain and jaundice. She had a reagent antinuclear factor (1:640, with a homogeneous nuclear pattern) and hypergammaglobulinemia (2.16 g/dL). Anti-smooth muscle, anti-mitochondrial and anti-liver-kidney microsomal antibody type 1 antibodies were negative. Magnetic resonance cholangiography showed a cirrhotic liver with multiple focal areas of strictures of the intrahepatic bile ducts, with associated dilations. Liver biopsy demonstrated periportal necroinflammatory activity, plasmocyte infiltration and advanced fibrosis. Colonoscopy showed ulcerative pancolitis and mild activity (Mayo score 1), with a spared rectum. Treatment with corticosteroids, azathioprine, ursodeoxycholic acid and mesalamine was initiated, with improvement in laboratory tests. The patient was referred for a liver transplantation evaluation.
Aim: To report the case of a female patient with autoimmune hepatitis and primary sclerosing cholangitis (PSC) overlap syndrome associated with ulcerative colitis and to systematically review the available cases of autoimmune hepatitis and PSC overlap syndrome.
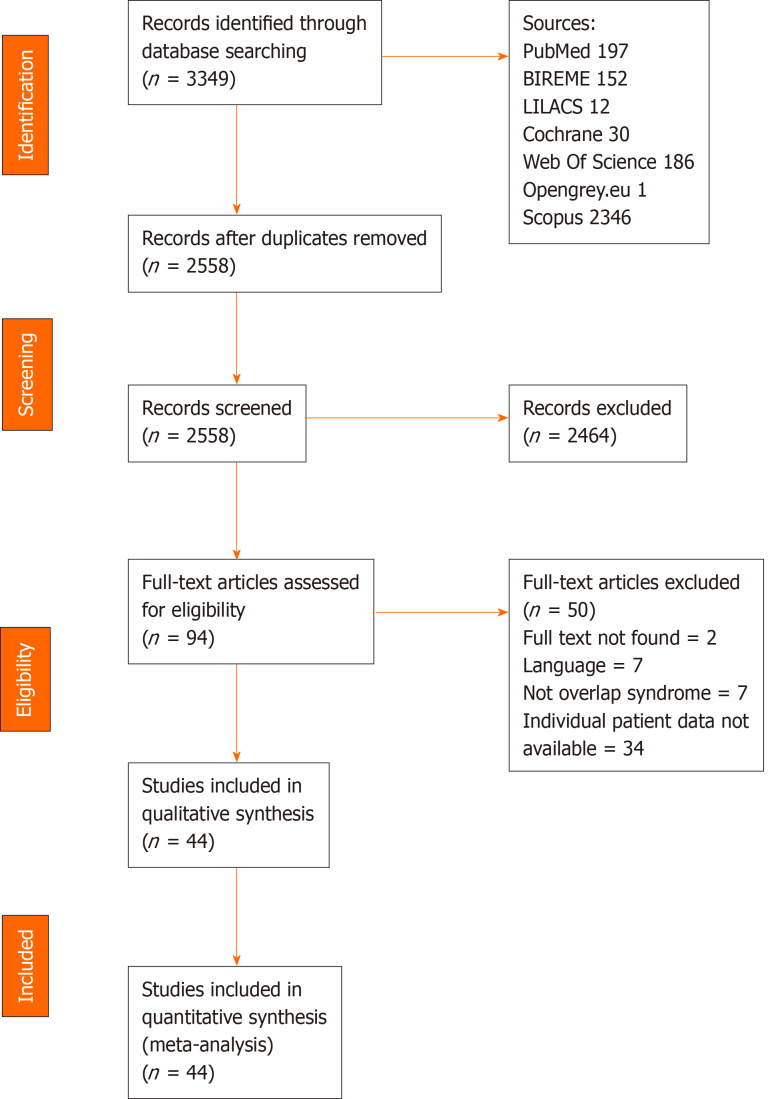
Methods: In accordance with preferred reporting items for systematic reviews and meta-analysis protocols guidelines, retrieval of studies was based on medical subject headings and health sciences descriptors, which were combined using Boolean operators. Searches were run on the electronic databases Scopus, Web of Science, MEDLINE (PubMed), Biblioteca Regional de Medicina, Latin American and Caribbean Health Sciences Literature, Cochrane Library for Systematic Reviews and Opengray.eu. Languages were restricted to English, Spanish and Portuguese. There was no date of publication restrictions. The reference lists of the studies retrieved were searched manually.
Results: The search strategy retrieved 3349 references. In the final analysis, 44 references were included, with a total of 109 cases reported. The most common clinical finding was jaundice and 43.5% of cases were associated with inflammatory bowel disease. Of these, 27.6% were cases of Crohn's disease, 68% of ulcerative colitis, and 6.4% of indeterminate colitis. Most patients were treated with steroids. All-cause mortality was 3.7%.
Conclusion: PSC and autoimmune hepatitis overlap syndrome is generally associated with inflammatory bowel disease and has low mortality and good response to treatment.
Keywords: Autoimmune hepatitis; Crohn’s disease; Inflammatory bowel diseases; Primary sclerosing cholangitis; Ulcerative colitis.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors declare that they have no competing interests.
Figures
Similar articles
-
Hemophagocytic Lymphohistiocytosis and Inflammatory Bowel Disease: Case Report and Systematic Review.Inflamm Intest Dis. 2020 Jun;5(2):49-58. doi: 10.1159/000506514. Epub 2020 Mar 10. Inflamm Intest Dis. 2020. PMID: 32596254 Free PMC article. Review.
-
Autoimmune diseases of the liver and biliary tract and overlap syndromes in childhood.Minerva Gastroenterol Dietol. 2009 Mar;55(1):53-70. Minerva Gastroenterol Dietol. 2009. PMID: 19212308 Review.
-
Overlap syndrome between autoimmune hepatitis and primary sclerosing cholangitis in two cases.Eur J Gastroenterol Hepatol. 2000 May;12(5):559-64. doi: 10.1097/00042737-200012050-00014. Eur J Gastroenterol Hepatol. 2000. PMID: 10833101
-
Intestinal Paracoccidioidomycosis: Case report and systematic review.Braz J Infect Dis. 2021 Jul-Aug;25(4):101605. doi: 10.1016/j.bjid.2021.101605. Epub 2021 Aug 27. Braz J Infect Dis. 2021. PMID: 34461048 Free PMC article.
-
Generalized Pyoderma Gangrenosum Associated with Ulcerative Colitis: Successful Treatment with Infliximab and Azathioprine.Acta Dermatovenerol Croat. 2016 Apr;24(1):83-5. Acta Dermatovenerol Croat. 2016. PMID: 27149138
Cited by
-
Chronic Viral Hepatitis in a Cohort of Inflammatory Bowel Disease Patients from Southern Italy: A Case-Control Study.Pathogens. 2020 Oct 23;9(11):870. doi: 10.3390/pathogens9110870. Pathogens. 2020. PMID: 33113974 Free PMC article.
-
Overlap syndromes in autoimmune liver disease: a review.Transl Gastroenterol Hepatol. 2025 Apr 15;10:33. doi: 10.21037/tgh-24-140. eCollection 2025. Transl Gastroenterol Hepatol. 2025. PMID: 40337770 Free PMC article. Review.
-
Hepatobiliary manifestations in inflammatory bowel disease: A practical approach.World J Hepatol. 2022 Feb 27;14(2):319-337. doi: 10.4254/wjh.v14.i2.319. World J Hepatol. 2022. PMID: 35317174 Free PMC article. Review.
-
Risk and management of post-operative infectious complications in inflammatory bowel disease: A systematic review.World J Gastrointest Surg. 2023 Nov 27;15(11):2579-2595. doi: 10.4240/wjgs.v15.i11.2579. World J Gastrointest Surg. 2023. PMID: 38111772 Free PMC article.
-
Ulcerative colitis complicated by primary sclerosing cholangitis and autoimmune hepatitis overlap syndrome: a case report and literature review.Front Immunol. 2023 May 9;14:1132072. doi: 10.3389/fimmu.2023.1132072. eCollection 2023. Front Immunol. 2023. PMID: 37228618 Free PMC article. Review.
References
-
- Czaja AJ, Manns MP. Advances in the diagnosis, pathogenesis, and management of autoimmune hepatitis. Gastroenterology. 2010;139:58–72.e4. - PubMed
-
- Wurbs D, Klein R, Terracciano LM, Berg PA, Bianchi L. A 28-year-old woman with a combined hepatitic/cholestatic syndrome. Hepatology. 1995;22:1598–1605. - PubMed
-
- Lawrence SP, Sherman KE, Lawson JM, Goodman ZD. A 39 year old man with chronic hepatitis. Semin Liver Dis. 1994;14:97–105. - PubMed
LinkOut - more resources
Full Text Sources
