

Randomized Trial Evaluation of the Benefits and Risks of Menopausal Hormone Therapy Among Women 50-59 Years of Age
- PMID: 33025002
- PMCID: PMC8086238
- DOI: 10.1093/aje/kwaa210
Randomized Trial Evaluation of the Benefits and Risks of Menopausal Hormone Therapy Among Women 50-59 Years of Age
Abstract
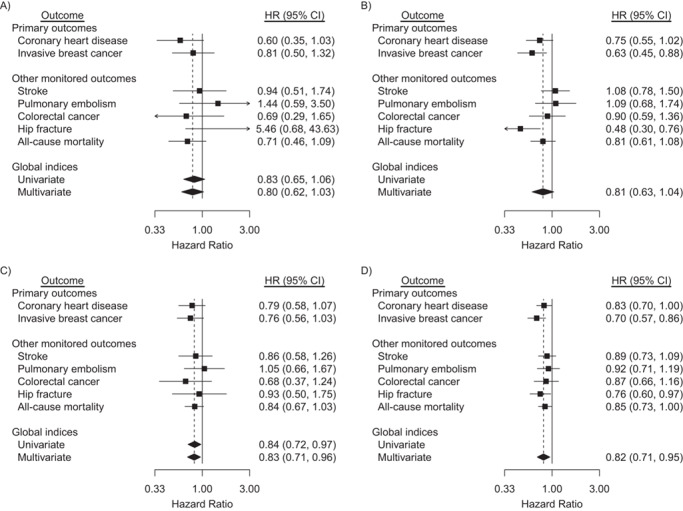
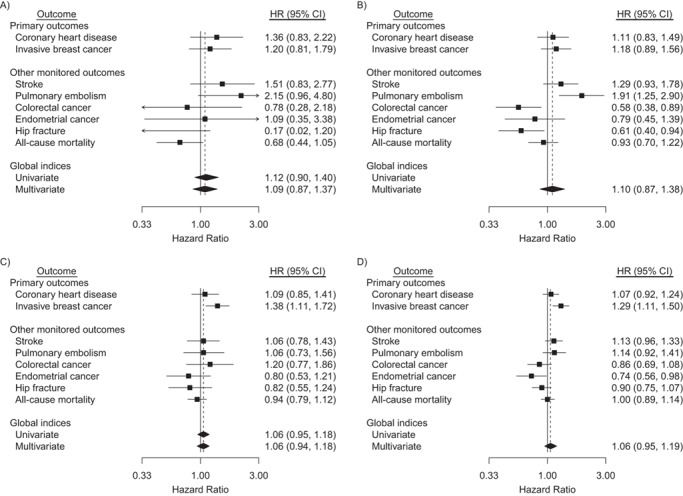
The health benefits and risks of menopausal hormone therapy among women aged 50-59 years are examined in the Women's Health Initiative randomized, placebo-controlled trials using long-term follow-up data and a parsimonious statistical model that leverages data from older participants to increase precision. These trials enrolled 27,347 healthy postmenopausal women aged 50-79 years at 40 US clinical centers during 1993-1998, including 10,739 post-hysterectomy participants in a trial of conjugated equine estrogens and 16,608 participants with a uterus in the trial of these estrogens plus medroxyprogesterone acetate. Over a (median) 18-year follow-up period (1993-2016), risk for a global index (defined as the earliest of coronary heart disease, invasive breast cancer, stroke, pulmonary embolism, colorectal cancer, endometrial cancer, hip fracture, and all-cause mortality) was reduced with conjugated equine estrogens with a hazard ratio of 0.82 (95% confidence interval: 0.71, 0.95), and with nominally significant reductions for coronary heart disease, breast cancer, hip fracture, and all-cause mortality. Corresponding global index hazard ratio estimates of 1.06 (95% confidence interval: 0.95, 1.19) were nonsignificant for combined estrogens plus progestin, but increased breast cancer risk and reduced endometrial cancer risk were observed. These results, among women 50-59 years of age, substantially agree with the worldwide observational literature, with the exception of breast cancer for estrogens alone.
Keywords: benefits versus risks; estrogens; global index; hazard ratio; menopausal hormone therapy; multivariate failure times; progestin.
Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health 2020. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
References
-
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–333. - PubMed
-
- Ettinger B, Wang SM, Scott LR, et al. Evolution of postmenopausal hormone therapy between 2002 and 2009. Menopause. 2012;19(6):610–615. - PubMed
-
- Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogens in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701–1712. - PubMed
