

Myocarditis: imaging up to date
- PMID: 33025305
- PMCID: PMC7538190
- DOI: 10.1007/s11547-020-01279-8
Myocarditis: imaging up to date
Abstract
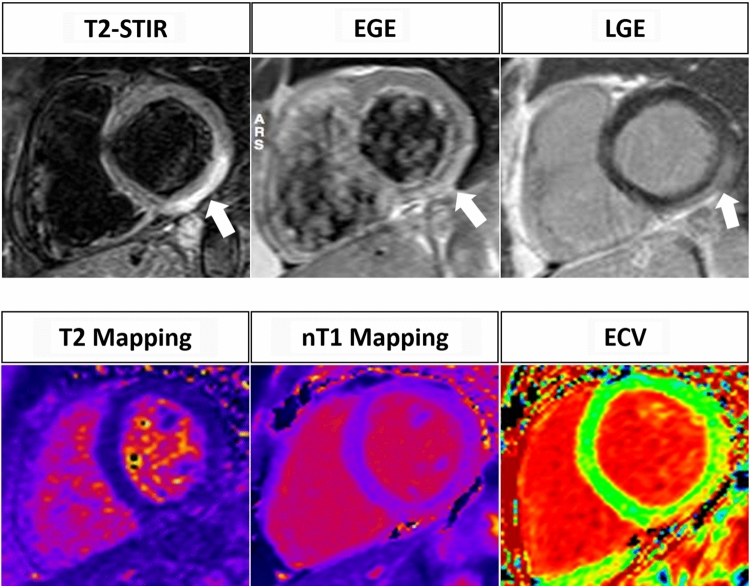
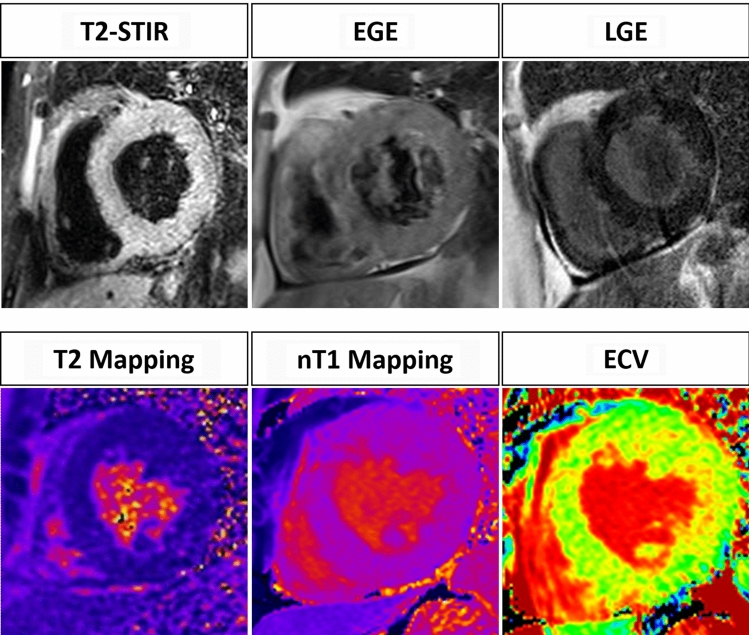
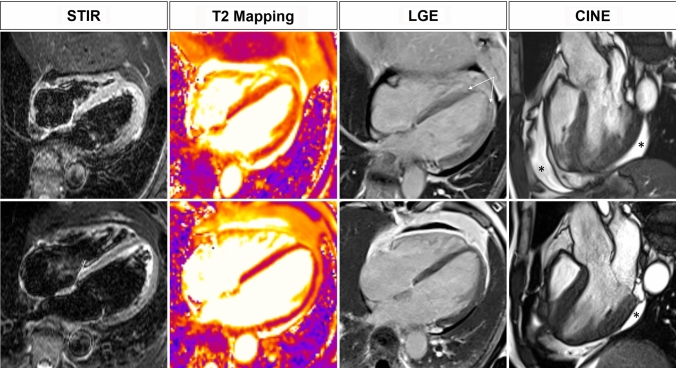
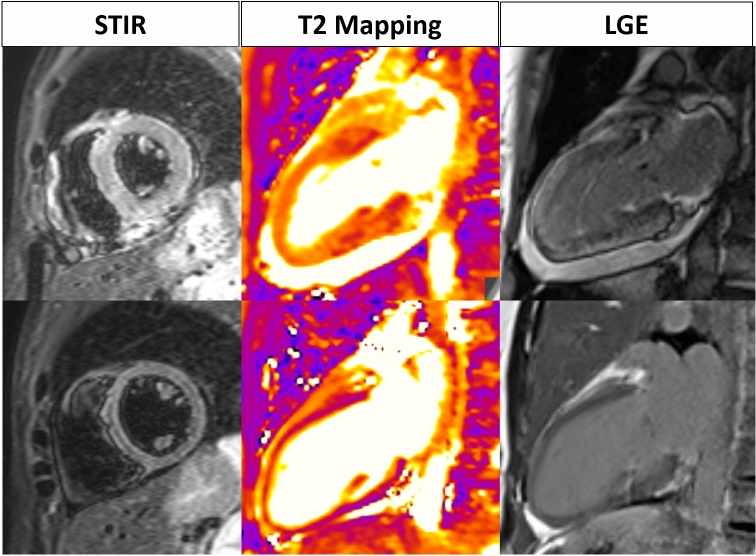
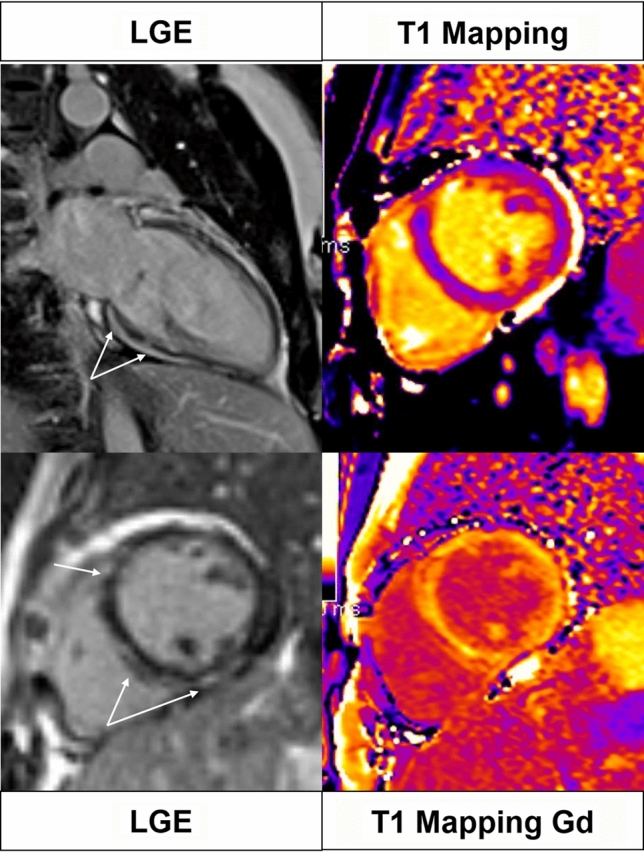
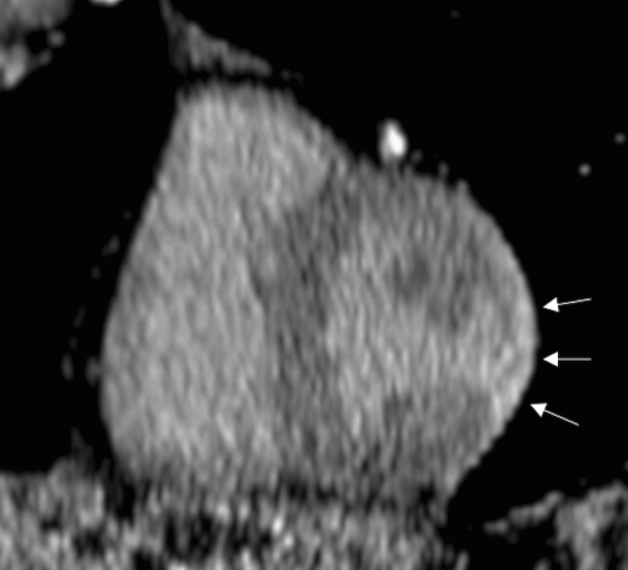
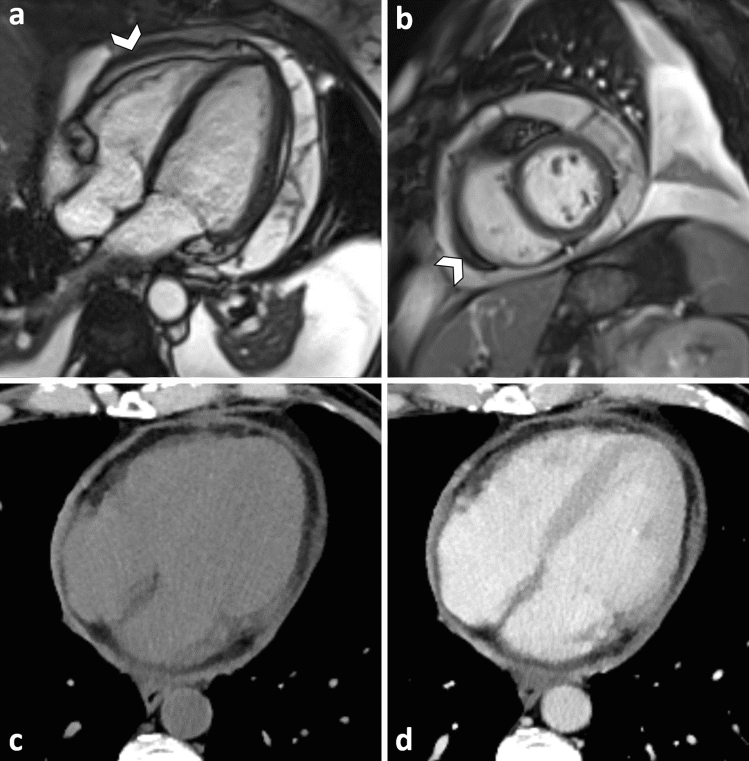
Myocarditis is an inflammatory disease of the heart muscle, diagnosed by histological, immunological, and immunohistochemical criteria. Endomyocardial biopsy represents the diagnostic gold standard for its diagnosis but is infrequently used. Due to its noninvasive ability to detect the presence of myocardial edema, hyperemia and necrosis/fibrosis, Cardiac MR imaging is routinely used in the clinical practice for the diagnosis of acute myocarditis. Recently pixel-wise mapping of T1 and T2 relaxation time have been introduced into the clinical Cardiac MR protocol increasing its accuracy. Our paper will review the role of MR imaging in the diagnosis of acute myocarditis.
Keywords: Cardiac MR; Magnetic resonance imaging; Myocardial inflammation; Myocarditis.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Monney P, Locca D, Muzzarelli S, et al. Cardiac magnetic resonance in acute myocarditis: A new non-invasive diagnostic gold standard? Rev Med Suisse. 2012;8(343):1177–1183. - PubMed
-
- Caforio AL, Pankuweit S, Arbustini E, et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of a position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur Heart J. 2013;34:2636–2648d. doi: 10.1093/eurheartj/eht210. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
