

Monitoring the Burden of Seizures and Highly Epileptiform Patterns in Critical Care with a Novel Machine Learning Method
- PMID: 33025543
- PMCID: PMC8021593
- DOI: 10.1007/s12028-020-01120-0
Monitoring the Burden of Seizures and Highly Epileptiform Patterns in Critical Care with a Novel Machine Learning Method
Abstract
Introduction: Current electroencephalography (EEG) practice relies on interpretation by expert neurologists, which introduces diagnostic and therapeutic delays that can impact patients' clinical outcomes. As EEG practice expands, these experts are becoming increasingly limited resources. A highly sensitive and specific automated seizure detection system would streamline practice and expedite appropriate management for patients with possible nonconvulsive seizures. We aimed to test the performance of a recently FDA-cleared machine learning method (Claritγ, Ceribell Inc.) that measures the burden of seizure activity in real time and generates bedside alerts for possible status epilepticus (SE).
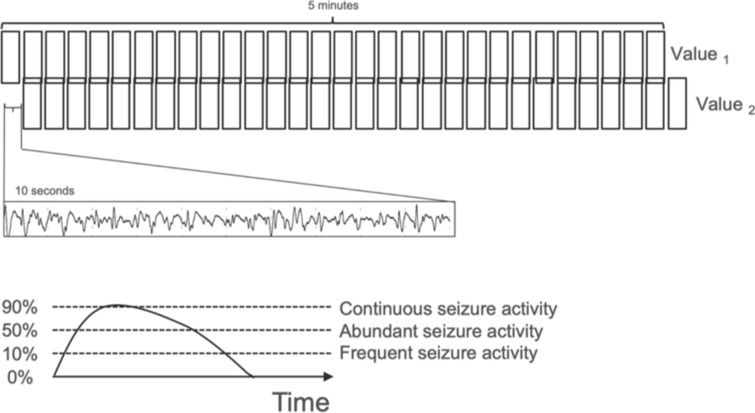
Methods: We retrospectively identified adult patients (n = 353) who underwent evaluation of possible seizures with Rapid Response EEG system (Rapid-EEG, Ceribell Inc.). Automated detection of seizure activity and seizure burden throughout a recording (calculated as the percentage of ten-second epochs with seizure activity in any 5-min EEG segment) was performed with Claritγ, and various thresholds of seizure burden were tested (≥ 10% indicating ≥ 30 s of seizure activity in the last 5 min, ≥ 50% indicating ≥ 2.5 min of seizure activity, and ≥ 90% indicating ≥ 4.5 min of seizure activity and triggering a SE alert). The sensitivity and specificity of Claritγ's real-time seizure burden measurements and SE alerts were compared to the majority consensus of at least two expert neurologists.
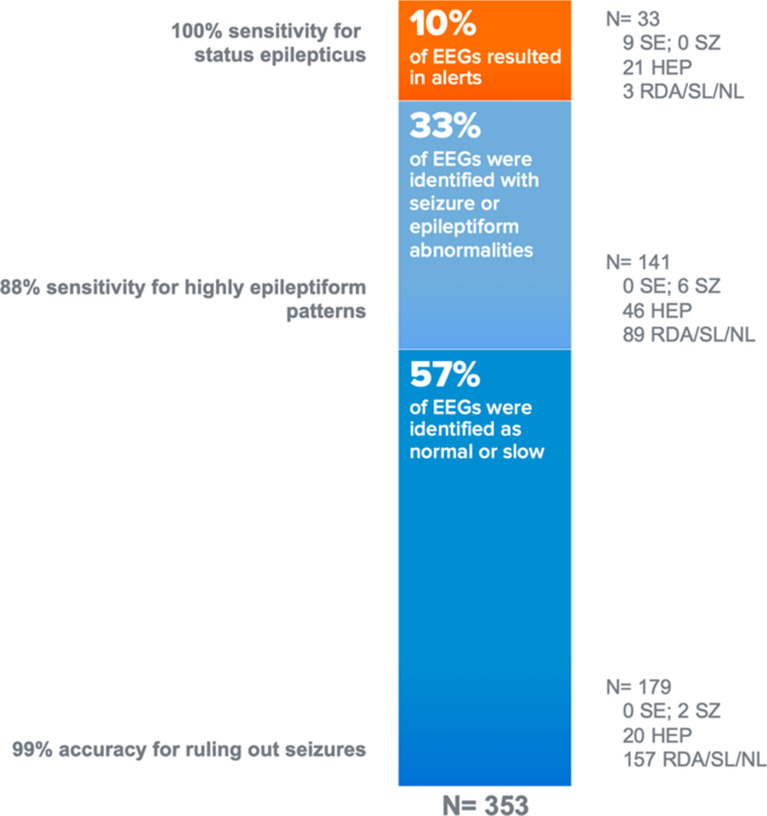
Results: Majority consensus of neurologists labeled the 353 EEGs as normal or slow activity (n = 249), highly epileptiform patterns (HEP, n = 87), or seizures [n = 17, nine longer than 5 min (e.g., SE), and eight shorter than 5 min]. The algorithm generated a SE alert (≥ 90% seizure burden) with 100% sensitivity and 93% specificity. The sensitivity and specificity of various thresholds for seizure burden during EEG recordings for detecting patients with seizures were 100% and 82% for ≥ 50% seizure burden and 88% and 60% for ≥ 10% seizure burden. Of the 179 EEG recordings in which the algorithm detected no seizures, seizures were identified by the expert reviewers in only two cases, indicating a negative predictive value of 99%.
Discussion: Claritγ detected SE events with high sensitivity and specificity, and it demonstrated a high negative predictive value for distinguishing nonepileptiform activity from seizure and highly epileptiform activity.
Conclusions: Ruling out seizures accurately in a large proportion of cases can help prevent unnecessary or aggressive over-treatment in critical care settings, where empiric treatment with antiseizure medications is currently prevalent. Claritγ's high sensitivity for SE and high negative predictive value for cases without epileptiform activity make it a useful tool for triaging treatment and the need for urgent neurological consultation.
Keywords: Electroencephalography; Machine learning method; Neurology; Seizure burden; Status epilepticus.
Conflict of interest statement
Drs. Decker, Khankhanian, and Mainardi have no conflicts of interest to declare. Drs. Kamousi, Karunakaran and Woo are members of research team at Ceribell (Mountain View, California) and developed the seizure burden algorithm. Drs. Gururangan, Markert, and Quinn serve as scientific advisers to Ceribell. Dr. Parvizi is main inventor of the EEG system discussed in this manuscript and co-founder of Ceribell. Dr. Quinn’s and Dr. Parvizi’s contributions to this publication were not part of their Stanford University duties or responsibilities.
Figures

References
-
- Betjemann JP, Lowenstein DH. Status epilepticus in adults. Lancet Neurol. 2015;14(6):615–624. - PubMed
-
- Kaplan PW. Nonconvulsive status epilepticus in the emergency room. Epilepsia. 1996;37(7):643–650. - PubMed
-
- Claassen J, Mayer SA, Kowalski RG, Emerson RG, Hirsch LJ. Detection of electrographic seizures with continuous EEG monitoring in critically ill patients. Neurology. 2004;62(10):1743–1748. - PubMed
-
- Claassen J, Jetté N, Chum F, Green R, Schmidt M, Choi H, Jirsch J, Frontera JA, Connolly ES, Emerson RG, et al. Electrographic seizures and periodic discharges after intracerebral hemorrhage. Neurology. 2007;69(13):1356–1365. - PubMed
-
- Rossetti AO, Logroscino G, Liaudet L, Ruffieux C, Ribordy V, Schaller MD, Despland PA, Oddo M. Status epilepticus: an independent outcome predictor after cerebral anoxia. Neurology. 2007;69(3):255–260. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
