

Examination of the Annular Tendon (Annulus of Zinn) as a Common Origin of the Extraocular Rectus Muscles: 2. Embryological Basis of Extraocular Muscles Anomalies
- PMID: 33026455
- PMCID: PMC7545067
- DOI: 10.1167/iovs.61.12.5
Examination of the Annular Tendon (Annulus of Zinn) as a Common Origin of the Extraocular Rectus Muscles: 2. Embryological Basis of Extraocular Muscles Anomalies
Abstract
Purpose: Many reports have described anomalous connections of the superior rectus (SR) with other extraocular rectus muscles, in which additional heads of the other three rectus muscles likely provided the connections. We examined how these connections are established during fetal development.
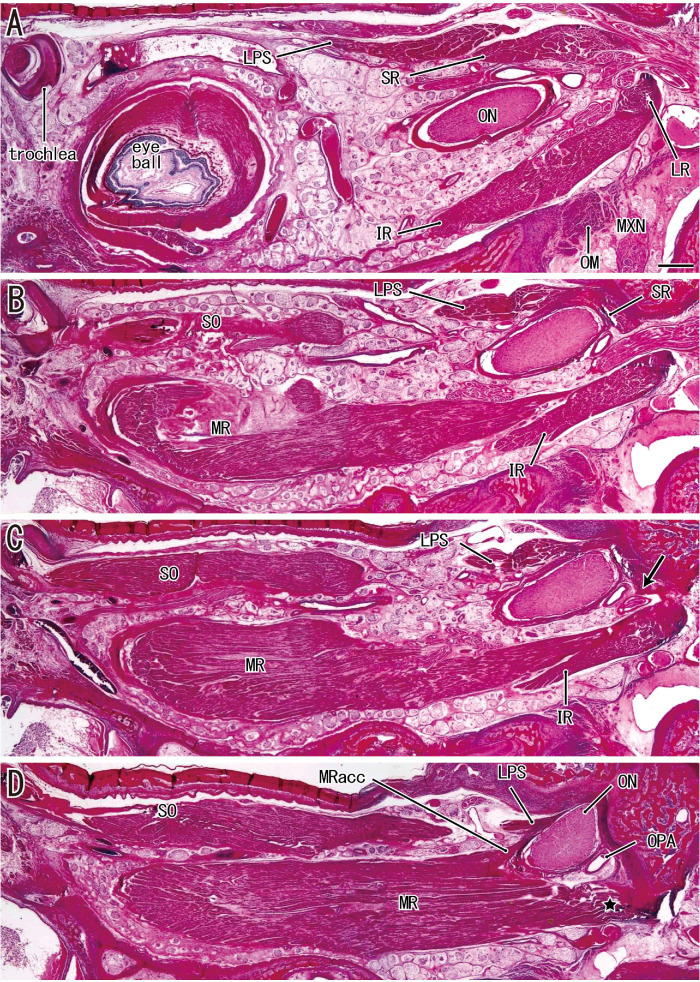
Methods: We analyzed paraffin-embedded horizontal sections from 25 late-stage fetuses. Horizontal sections are best suited for understanding the mediolateral relationships of muscle origins.
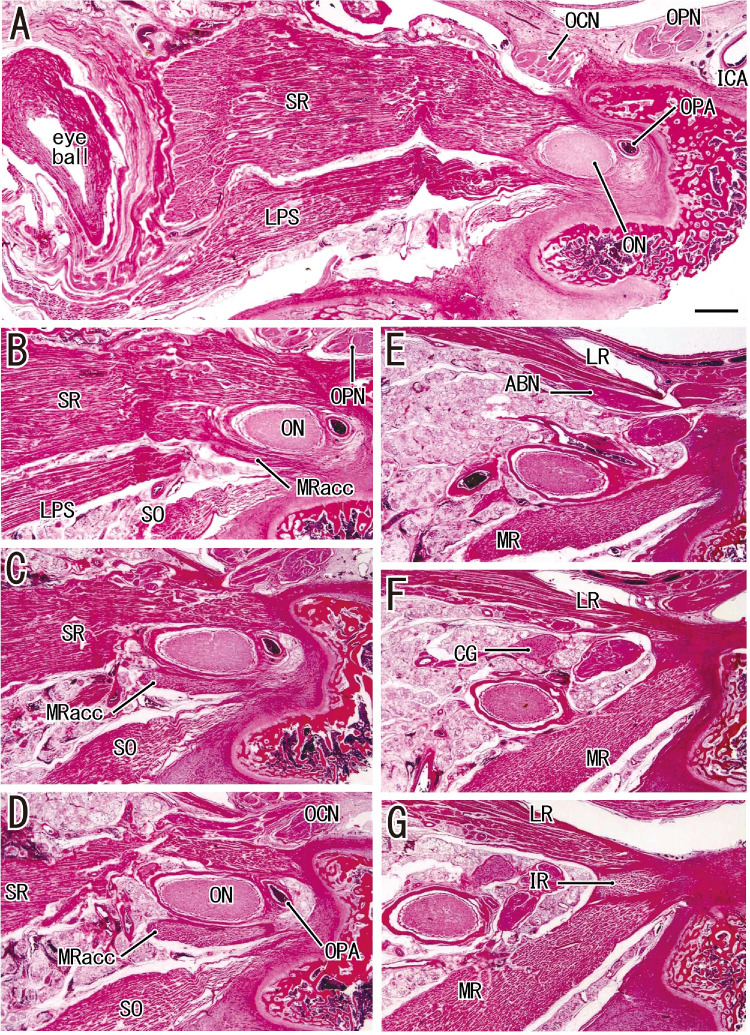
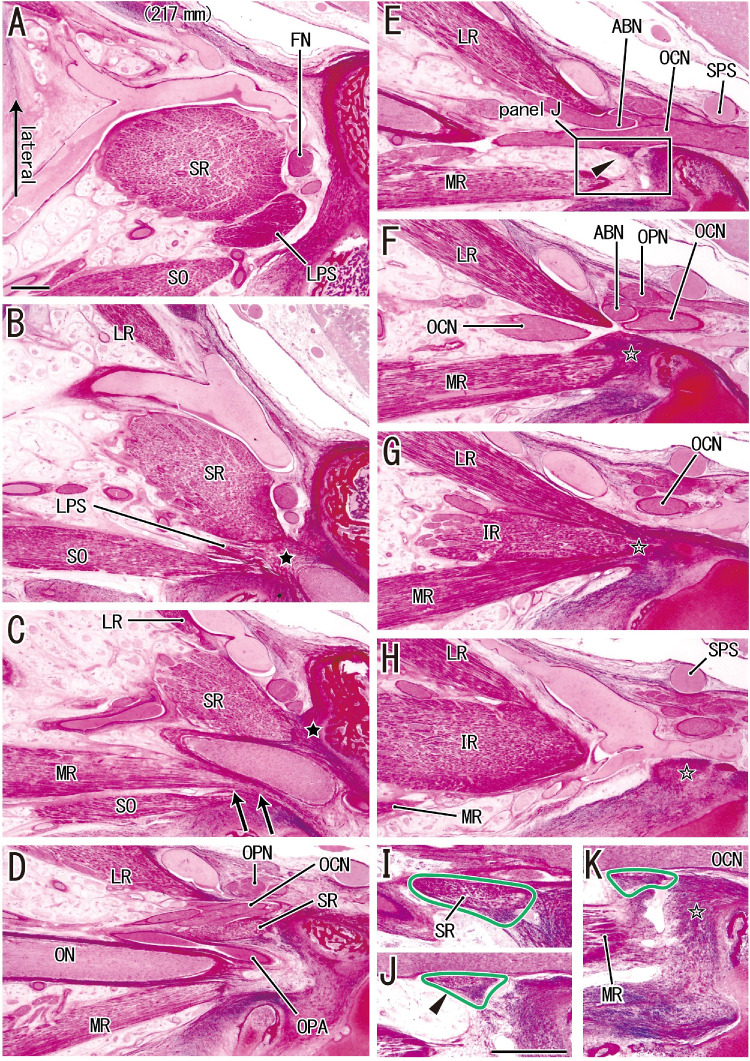
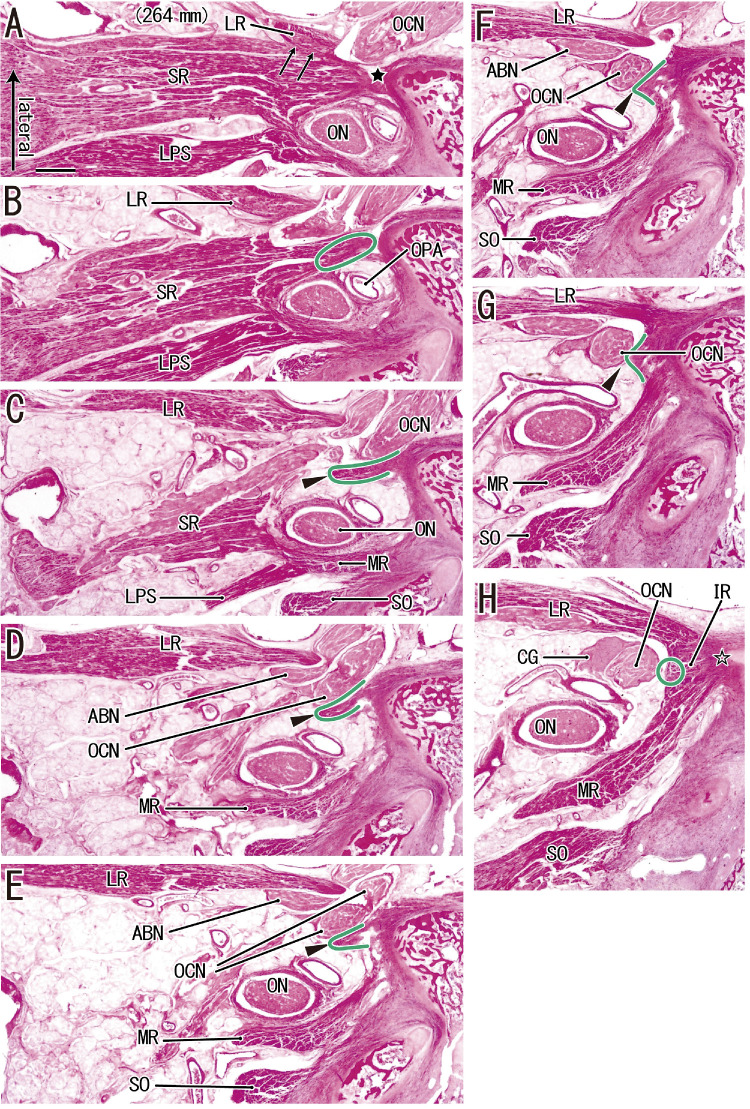
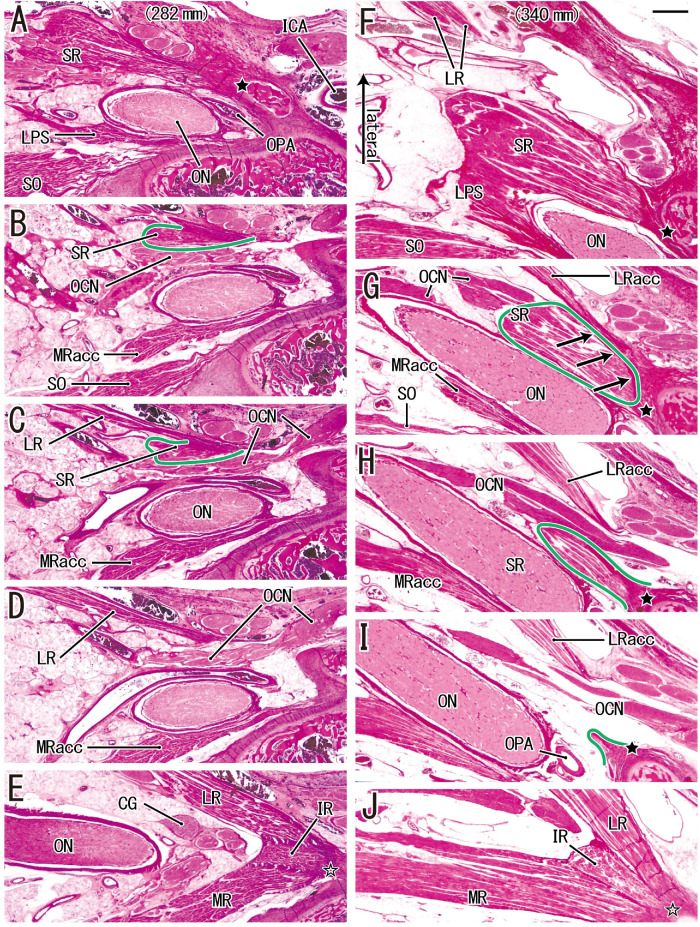
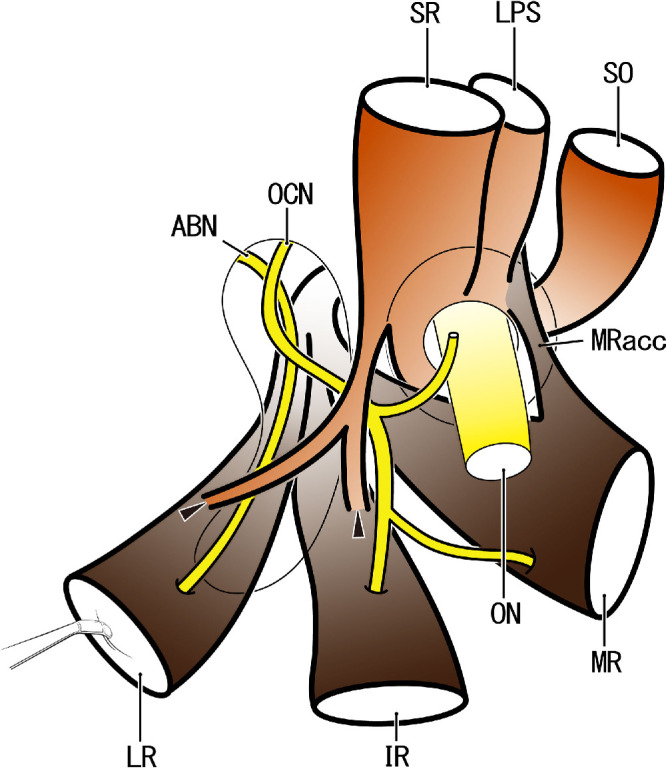
Results: We confirmed a common tendinous origin of the lateral rectus (LR), inferior rectus (IR) and medial rectus (MR) muscles that was separated from the SR origin. Notably, eight fetuses (32%) had tendinous or muscular connections between the SR and other rectus muscles that had one of four morphologies: (a) a thin tendon from the SR to the common tendon of the three rectus muscles (2 fetuses), (b) a thin tendon to the LR (one fetus), (c) a thin tendon to the inferior rectus muscle origin (two fetuses), and (d) SR muscle fibers arising from an additional head of the LR (three fetuses).
Conclusions: The SR seemed to issue a thin tendon that passed along the inferior or lateral side of the oculomotor nerve. Conversely, the LR and inferior rectus muscle were likely to carry a supernumerary bundle that reached the SR. The accessory head of the medial rectus muscle showed a stable morphology in that it seemed to also provide an anomalous double head. However, the presence of an accessory head in the LR was rare. In contrast with our previously published diagram of the orbital apex, the accessory head of the medial rectus muscle passed along the lateral side of the superior oblique.
Conflict of interest statement
Disclosure:
Figures
Similar articles
-
Examination of the Topographical Anatomy and Fetal Development of the Tendinous Annulus of Zinn for a Common Origin of the Extraocular Recti.Invest Ophthalmol Vis Sci. 2019 Nov 1;60(14):4564-4573. doi: 10.1167/iovs.19-28094. Invest Ophthalmol Vis Sci. 2019. PMID: 31675425
-
Tendinous annulus of Zinn for a common origin of the extraocular rectus muscles: a histological study of the orbital apex from donated elderly cadavers.Anat Sci Int. 2022 Sep;97(4):369-379. doi: 10.1007/s12565-022-00649-8. Epub 2022 Feb 14. Anat Sci Int. 2022. PMID: 35157253
-
The origins and insertions of the extraocular muscles: development, histologic features, and clinical significance.Trans Am Ophthalmol Soc. 1986;84:488-526. Trans Am Ophthalmol Soc. 1986. PMID: 3590478 Free PMC article.
-
Double insertions of extraocular rectus muscles in humans and the pulley theory.J Anat. 2005 Mar;206(3):295-306. doi: 10.1111/j.1469-7580.2005.00383.x. J Anat. 2005. PMID: 15733302 Free PMC article. Review.
-
[Accessory extraocular muscle-a case report and review].Zhonghua Yan Ke Za Zhi. 2011 Dec;47(12):1111-6. Zhonghua Yan Ke Za Zhi. 2011. PMID: 22336122 Review. Chinese.
Cited by
-
Topographical anatomy of the annulus of Zinn.Sci Rep. 2022 Jan 20;12(1):1064. doi: 10.1038/s41598-022-05178-y. Sci Rep. 2022. PMID: 35058545 Free PMC article.
-
Association between the developing sphenoid and adult morphology: A study using sagittal sections of the skull base from human embryos and fetuses.J Anat. 2021 Dec;239(6):1300-1317. doi: 10.1111/joa.13515. Epub 2021 Jul 15. J Anat. 2021. PMID: 34268732 Free PMC article.
-
Formation and Fixation of the Annulus of Zinn and Relation With Extraocular Muscles: A Plastinated Histologic Study and Its Clinical Significance.Invest Ophthalmol Vis Sci. 2022 Nov 1;63(12):16. doi: 10.1167/iovs.63.12.16. Invest Ophthalmol Vis Sci. 2022. PMID: 36355368 Free PMC article.
-
Supernumerary Extraocular Muscle: A Rare Cause of Atypical Restrictive Strabismus.Medicina (Kaunas). 2022 Nov 21;58(11):1691. doi: 10.3390/medicina58111691. Medicina (Kaunas). 2022. PMID: 36422229 Free PMC article.
References
-
- Haladaj R, Wysiadecki G, Tubbs RS, Topol M. Anatomical variations of the levator palpebrae supeioris, including observations on its innervation and intramuscular nerves’ distribution pattern. Ann Anat. 2020; 228: 151439. - PubMed
-
- von Lüdinghausen M. Bilateral supernumerary rectus muscles of the orbit. Clin Anat. 1998; 11: 271–277. - PubMed
-
- Kakizaki H, Zako M, Nakano T, Asamoto K, Miyaishi O, Iwaki M. An anomalous muscle linking superior and inferior rectus muscles in the orbit. Anat Sci Int. 2006; 81: 197–199. - PubMed
-
- Mather TR, Saunders RA.. Congenital absence of the superior rectus muscle: a case report. J Pediatr Ophthalmol Strabismus. 1987; 24: 291–295. - PubMed
-
- Zőller CC, Gräf M, Kaufmann H. Unilateral aplasia of a lateral rectus muscle. Lin Monbl Augenheikd. 2001; 218: 55–60. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
