Mortality difference between early-identified sepsis and late-identified sepsis
- PMID: 33028057
- PMCID: PMC7550810
- DOI: 10.15441/ceem.19.009
Mortality difference between early-identified sepsis and late-identified sepsis
Abstract
Objective: The aim of the study was to compare the mortality rates of patients with early-identified (EI) sepsis and late-identified (LI) sepsis.
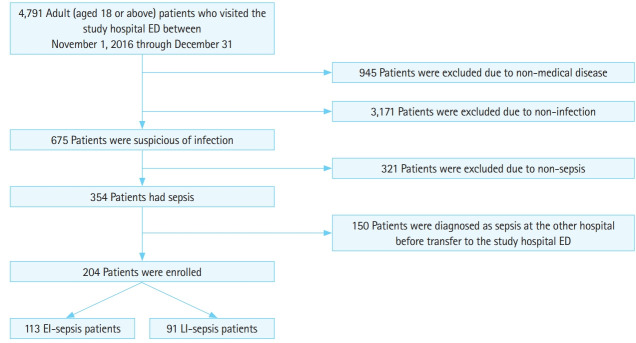
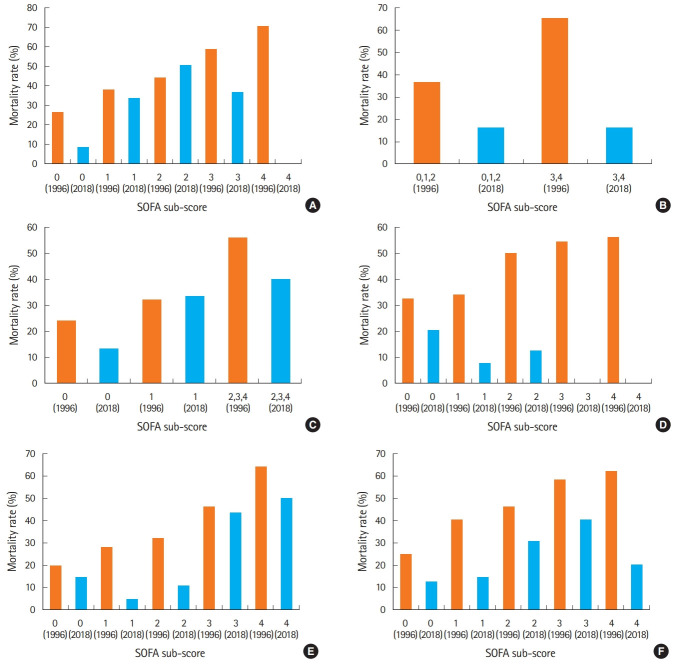
Methods: We performed a retrospective chart review of patients admitted to the emergency department and diagnosed with sepsis. EI sepsis was defined as patients with a Sequential Organ Failure Assessment (SOFA) score ≥2, based on 3 parameters of the SOFA score (Glasgow coma scale, mean arterial pressure, and partial pressure of oxygen/fraction of inspired oxygen ratio), measured within an hour of emergency department admission. The remaining patients were defined as LI sepsis. The primary outcome was in-hospital mortality.
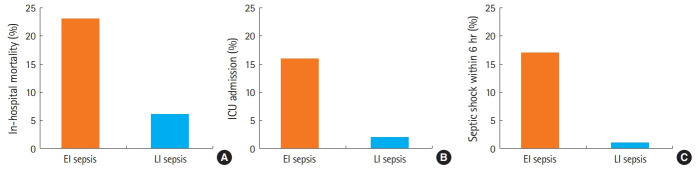
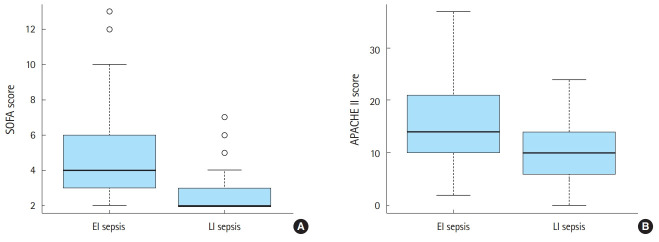
Results: Of the total 204 patients with sepsis, 113 (55.4%) had EI sepsis. Overall mortality rate was 15.7%, and EI sepsis group had significantly higher mortality than LI sepsis (23.0% vs. 6.6%, P=0.003). The patients with EI sepsis, compared to those with LI sepsis, had higher SOFA score (median: 4 vs. 2, P<0.001); Acute Physiology and Chronic Health Evaluation (APACHE) II score (median: 14 vs. 10, P<0.001); were more likely to progress to septic shock within 6 hours after admission (17.7% vs. 1.1%, P<0.001); were more likely to be admitted to the intensive care unit (2.2% vs. 1.1%, P=0.001).
Conclusion: Mortality was significantly higher in the EI sepsis group than in the LI sepsis group.
Keywords: Mortality; Sepsis; Shock, septic.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Similar articles
-
[Lactic acid, lactate clearance and procalcitonin in assessing the severity and predicting prognosis in sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020 Apr;32(4):449-453. doi: 10.3760/cma.j.cn121430-20200129-00086. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020. PMID: 32527351 Chinese.
-
[Predictive value of four different scoring systems for septic patient's outcome: a retrospective analysis with 311 patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017 Feb;29(2):133-138. doi: 10.3760/cma.j.issn.2095-4352.2017.02.008. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017. PMID: 28625260 Chinese.
-
[Assessment values of procalcitonin, lactic acid, and disease severity scores in patients with sepsis].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019 Aug;31(8):938-941. doi: 10.3760/cma.j.issn.2095-4352.2019.08.005. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019. PMID: 31537215 Chinese.
-
Prognostic scores for early stratification of septic patients admitted to an emergency department-high dependency unit.Eur J Emerg Med. 2014 Aug;21(4):254-9. doi: 10.1097/MEJ.0000000000000075. Eur J Emerg Med. 2014. PMID: 23970100
-
[Intestinal barrier dysfunction and its related factors in patients with sepsis].Zhonghua Yi Xue Za Zhi. 2016 Nov 29;96(44):3568-3572. doi: 10.3760/cma.j.issn.0376-2491.2016.44.007. Zhonghua Yi Xue Za Zhi. 2016. PMID: 27916077 Chinese.
Cited by
-
Association between Vitamin C Deficiency and Mortality in Patients with Septic Shock.Biomedicines. 2022 Aug 26;10(9):2090. doi: 10.3390/biomedicines10092090. Biomedicines. 2022. PMID: 36140190 Free PMC article.
-
Prediction of vasopressor requirement among hypotensive patients with suspected infection: usefulness of diastolic shock index and lactate.Clin Exp Emerg Med. 2022 Sep;9(3):176-186. doi: 10.15441/ceem.22.324. Epub 2022 Sep 30. Clin Exp Emerg Med. 2022. PMID: 36164800 Free PMC article.
-
Modified Cardiovascular Sequential Organ Failure Assessment Score in Sepsis: External Validation in Intensive Care Unit Patients.J Korean Med Sci. 2023 Dec 25;38(50):e418. doi: 10.3346/jkms.2023.38.e418. J Korean Med Sci. 2023. PMID: 38147839 Free PMC article.
-
Lipid nanoparticles from L. meyenii Walp mitigate sepsis through multimodal protein corona formation.Mol Ther Methods Clin Dev. 2025 May 14;33(2):101491. doi: 10.1016/j.omtm.2025.101491. eCollection 2025 Jun 12. Mol Ther Methods Clin Dev. 2025. PMID: 40496000 Free PMC article.
-
Timing and clinical risk factors for early acquisition of gut pathogen colonization with multidrug resistant organisms in the intensive care unit.Gut Pathog. 2024 Feb 21;16(1):10. doi: 10.1186/s13099-024-00605-z. Gut Pathog. 2024. PMID: 38383457 Free PMC article.
References
-
- Gilbert EH, Lowenstein SR, Koziol-McLain J, Barta DC, Steiner J. Chart reviews in emergency medicine research: Where are the methods? Ann Emerg Med. 1996;27:305–8. - PubMed
-
- Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–10. - PubMed
LinkOut - more resources
Full Text Sources