

Estimating the burden of HIV late presentation and its attributable morbidity and mortality across Europe 2010-2016
- PMID: 33028235
- PMCID: PMC7541282
- DOI: 10.1186/s12879-020-05261-7
Estimating the burden of HIV late presentation and its attributable morbidity and mortality across Europe 2010-2016
Abstract
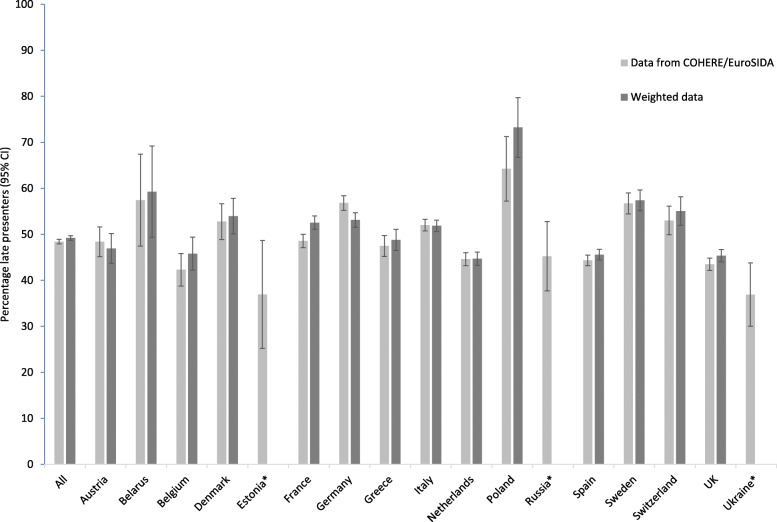
Background: Late presentation (LP), defined as a CD4 count < 350/mm3 or an AIDS-event at HIV-diagnosis, remains a significant problem across Europe. Linking cohort and surveillance data, we assessed the country-specific burden of LP during 2010-2016 and the occurrence of new AIDS events or deaths within 12 months of HIV-diagnosis believed to be attributable to LP.
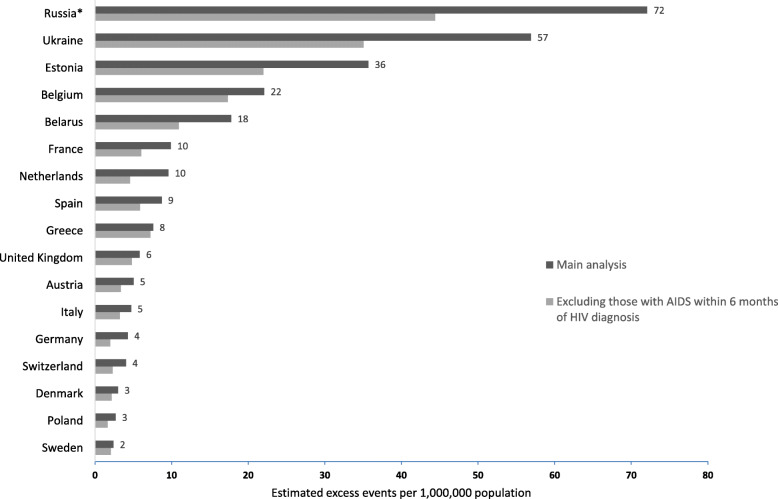
Methods: Country-specific percentages of LP and AIDS-events/death rates (assessed with Poisson regression) observed in The Collaboration of Observational HIV Epidemiological Research Europe (COHERE) and EuroSIDA cohorts, were applied to new HIV-diagnoses reported to the European Centre for Disease Prevention and Control. The estimated number of LP in the whole population was then calculated, as was the number of excess AIDS-events/deaths in the first 12 months following HIV-diagnosis assumed to be attributable to LP (difference in estimated events between LP and non-LP).
Results: Thirty-nine thousand two hundred four persons were included from the COHERE and EuroSIDA cohorts, of whom 18,967 (48.4%; 95% Confidence Interval [CI] 47.9-48.9) were classified as LP, ranging from 36.9% in Estonia (95%CI 25.2-48.7) and Ukraine (95%CI 30.0-43.8) to 64.2% in Poland (95%CI 57.2-71.3). We estimated a total of > 320,000 LP and 12,050 new AIDS-events/deaths attributable to LP during 2010-2016, with the highest estimated numbers of LP and excess AIDS-events/deaths in Eastern Europe. Country-level estimates of excess events ranged from 17 AIDS-events/deaths (95%CI 0-533) in Denmark to 10,357 (95%CI 7768-147,448) in Russia.
Conclusions: Across countries in Europe, the burden of LP was high, with the highest estimated number of LP and excess AIDS-events/deaths being in Eastern Europe. Effective strategies are needed to reduce LP and the attributable morbidity and mortality that could be potentially avoided.
Keywords: AIDS; Avoidable events; Eastern Europe; HIV; HIV testing; Late presentation.
Conflict of interest statement
All authors declare no conflicts of interest related to this article.
Figures
References
-
- World Health Organization. Guideline on when to start antiretroviral therapy and on pre-exposure prophylaxis for HIV. https://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en/. Accessed 12 Jan 2020. - PubMed
-
- World Health Organisation. Consolidated guidelines on HIV testing services. https://www.who.int/hiv/pub/guidelines/hiv-testing-services/en/. Accessed 12 Jan 2020.
-
- Mocroft A, Lundgren J, Antinori A, Monforte AD, Brännström J, Bonnet F, et al. Late presentation for HIV care across Europe: update from the collaboration of observational HIV epidemiological research Europe (COHERE) study, 2010 to 2013. Eurosurveillance. 2015;20(47). - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
