

Effect of school closures on mortality from coronavirus disease 2019: old and new predictions
- PMID: 33028597
- PMCID: PMC7536648
- DOI: 10.1136/bmj.m3588
Effect of school closures on mortality from coronavirus disease 2019: old and new predictions
Abstract
Objective: To replicate and analyse the information available to UK policymakers when the lockdown decision was taken in March 2020 in the United Kingdom.
Design: Independent calculations using the CovidSim code, which implements Imperial College London's individual based model, with data available in March 2020 applied to the coronavirus disease 2019 (covid-19) epidemic.
Setting: Simulations considering the spread of covid-19 in Great Britain and Northern Ireland.
Population: About 70 million simulated people matched as closely as possible to actual UK demographics, geography, and social behaviours.
Main outcome measures: Replication of summary data on the covid-19 epidemic reported to the UK government Scientific Advisory Group for Emergencies (SAGE), and a detailed study of unpublished results, especially the effect of school closures.
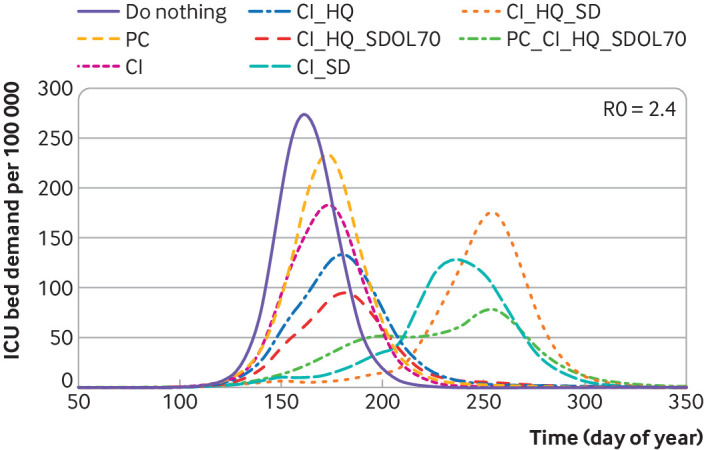
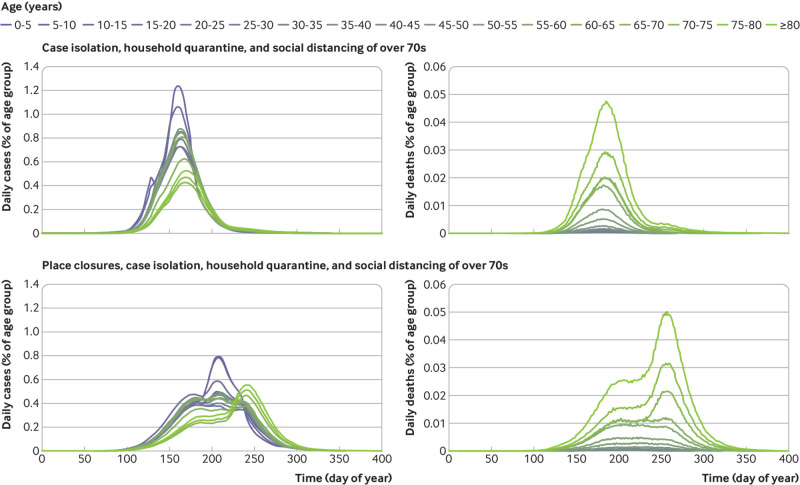
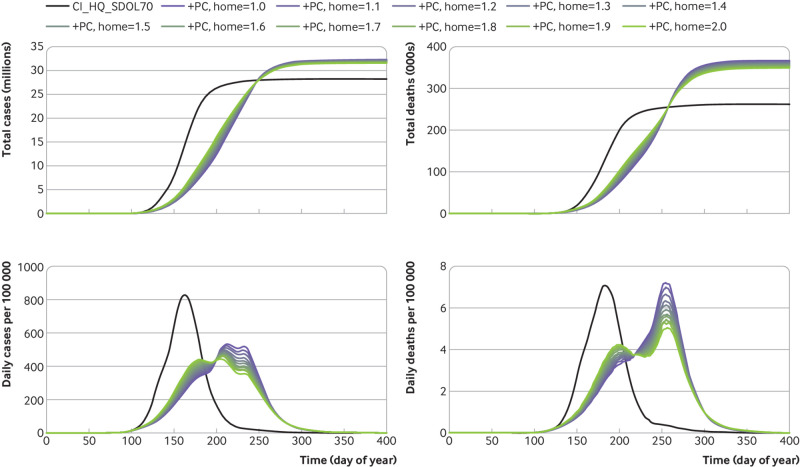
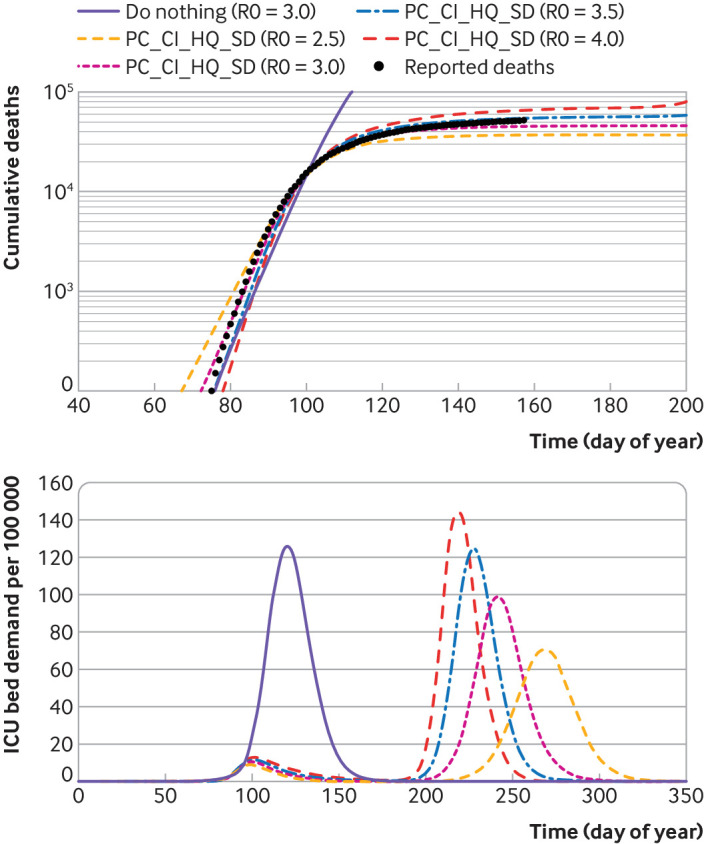
Results: The CovidSim model would have produced a good forecast of the subsequent data if initialised with a reproduction number of about 3.5 for covid-19. The model predicted that school closures and isolation of younger people would increase the total number of deaths, albeit postponed to a second and subsequent waves. The findings of this study suggest that prompt interventions were shown to be highly effective at reducing peak demand for intensive care unit (ICU) beds but also prolong the epidemic, in some cases resulting in more deaths long term. This happens because covid-19 related mortality is highly skewed towards older age groups. In the absence of an effective vaccination programme, none of the proposed mitigation strategies in the UK would reduce the predicted total number of deaths below 200 000.
Conclusions: It was predicted in March 2020 that in response to covid-19 a broad lockdown, as opposed to a focus on shielding the most vulnerable members of society, would reduce immediate demand for ICU beds at the cost of more deaths long term. The optimal strategy for saving lives in a covid-19 epidemic is different from that anticipated for an influenza epidemic with a different mortality age profile.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: support from UK Research and Innovation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Predicting the pandemic.BMJ. 2020 Oct 12;371:m3932. doi: 10.1136/bmj.m3932. BMJ. 2020. PMID: 33046438 No abstract available.
References
-
- Ferguson NM. Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand. Imperial College London; 2020. https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/covid-.... - PMC - PubMed
-
- Grewelle R, De Leo G. Estimating the global infection fatality rate of covid-19. medRxiv 2020. 10.1101/2020.05.11.20098780. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources