

ICOSL+ plasmacytoid dendritic cells as inducer of graft-versus-host disease, responsive to a dual ICOS/CD28 antagonist
- PMID: 33028709
- PMCID: PMC7811191
- DOI: 10.1126/scitranslmed.aay4799
ICOSL+ plasmacytoid dendritic cells as inducer of graft-versus-host disease, responsive to a dual ICOS/CD28 antagonist
Abstract
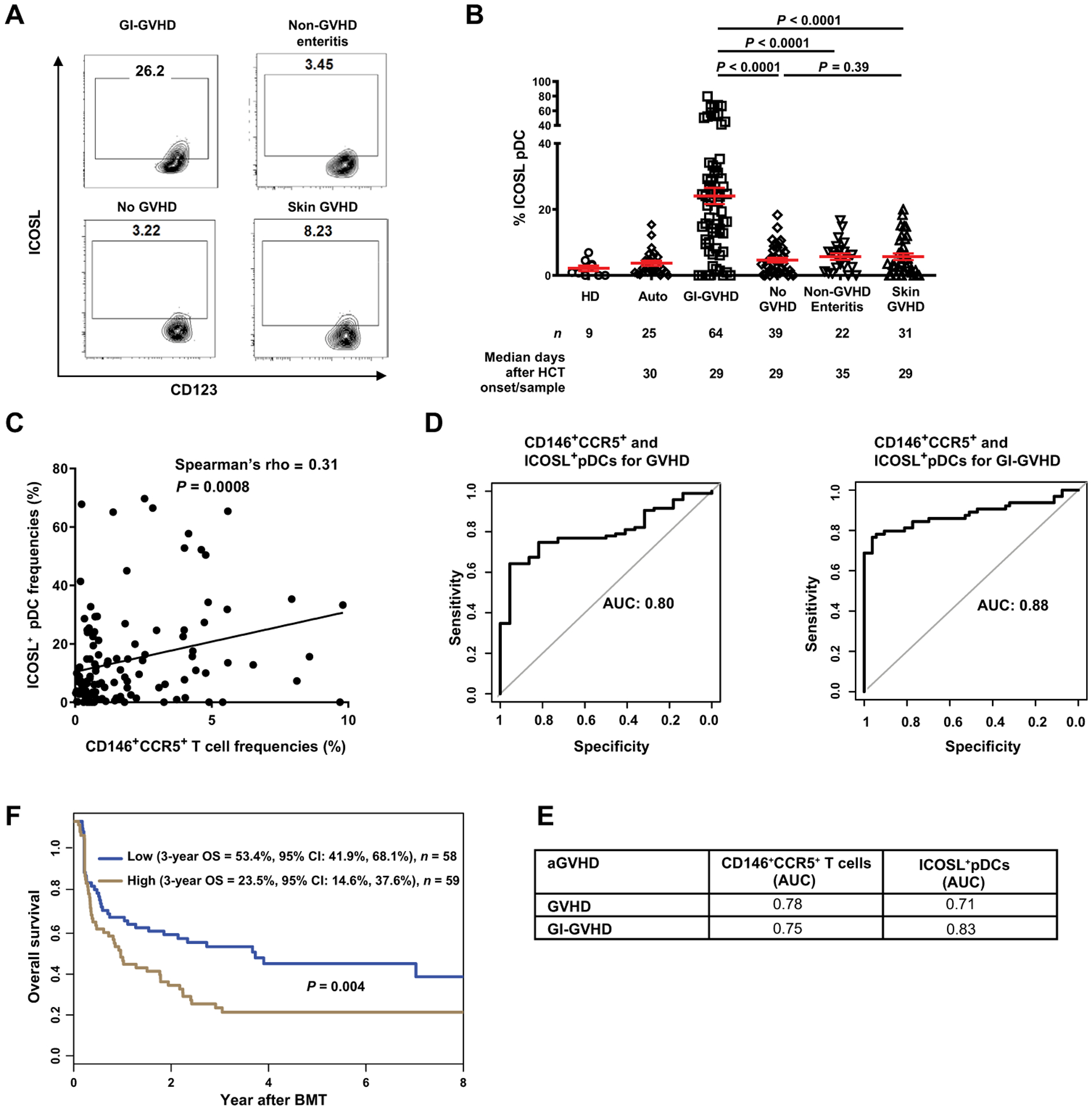
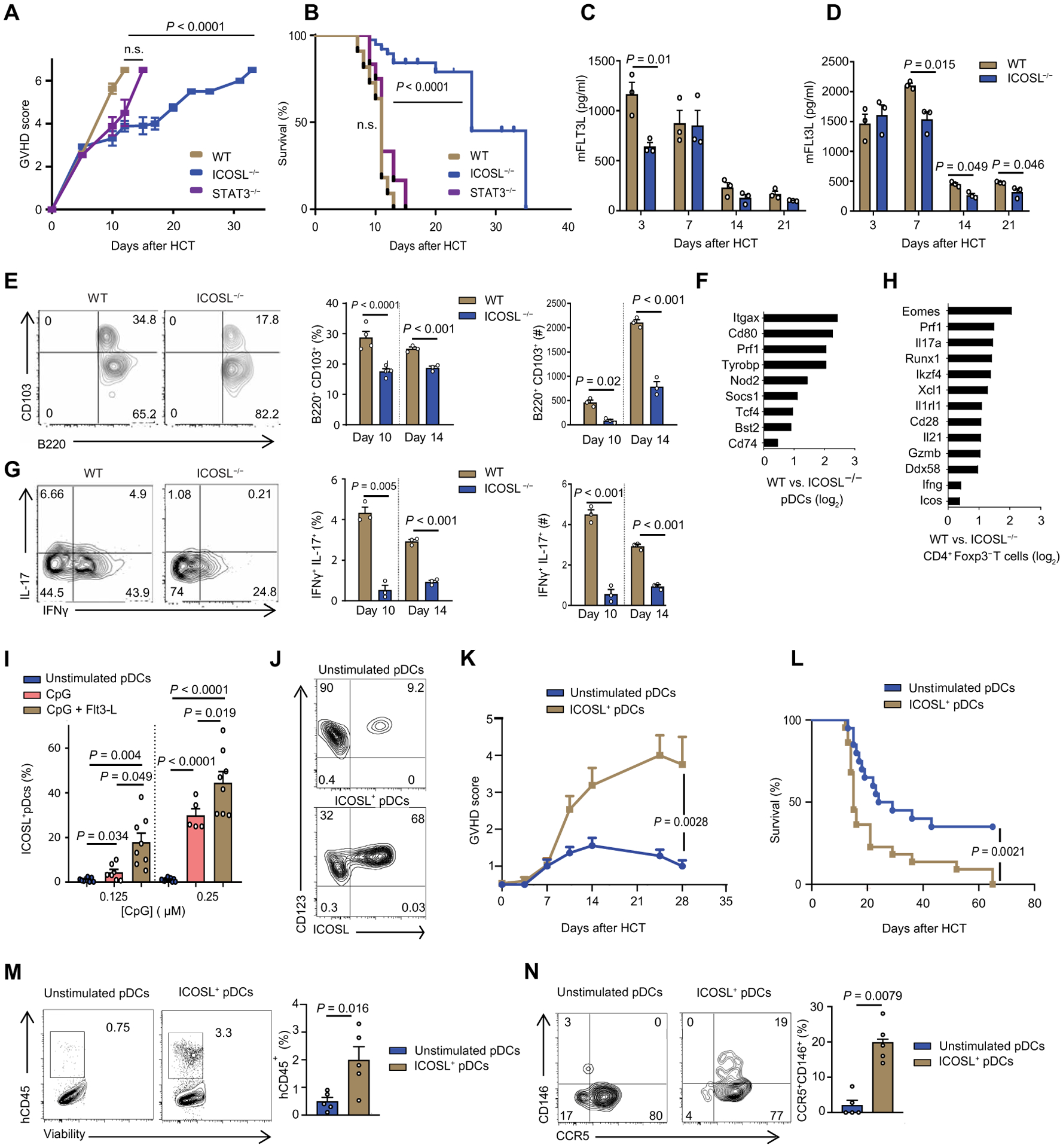
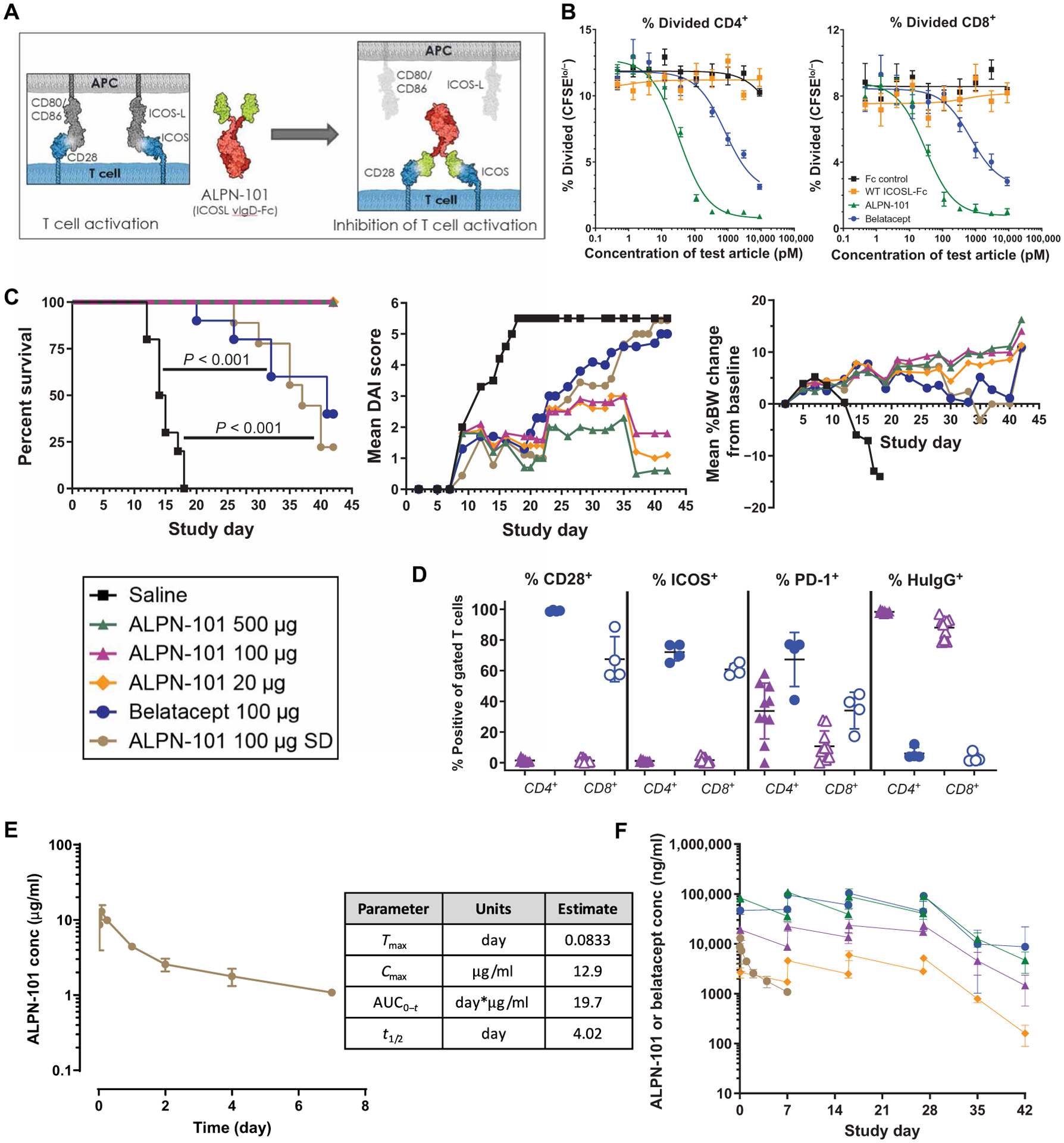
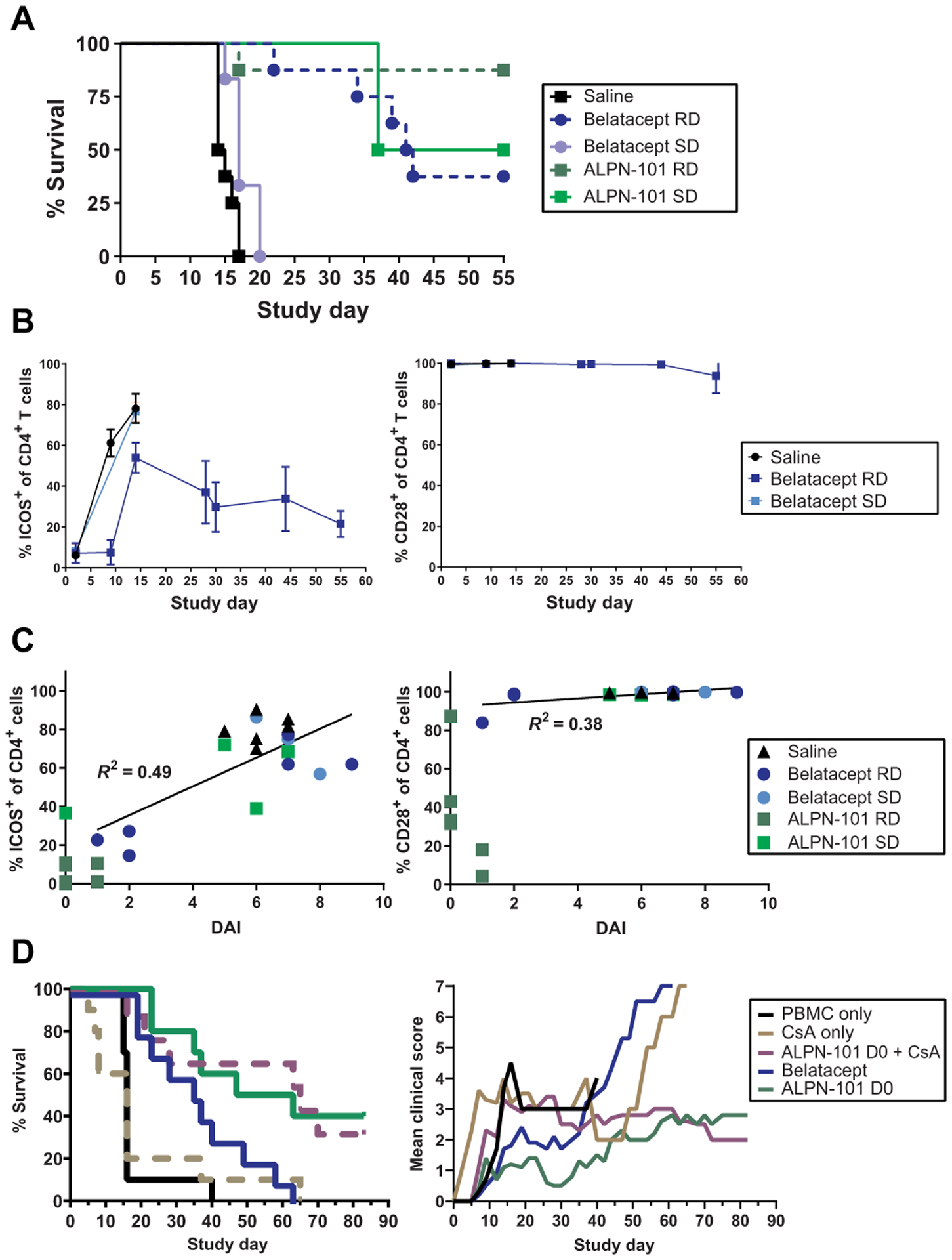
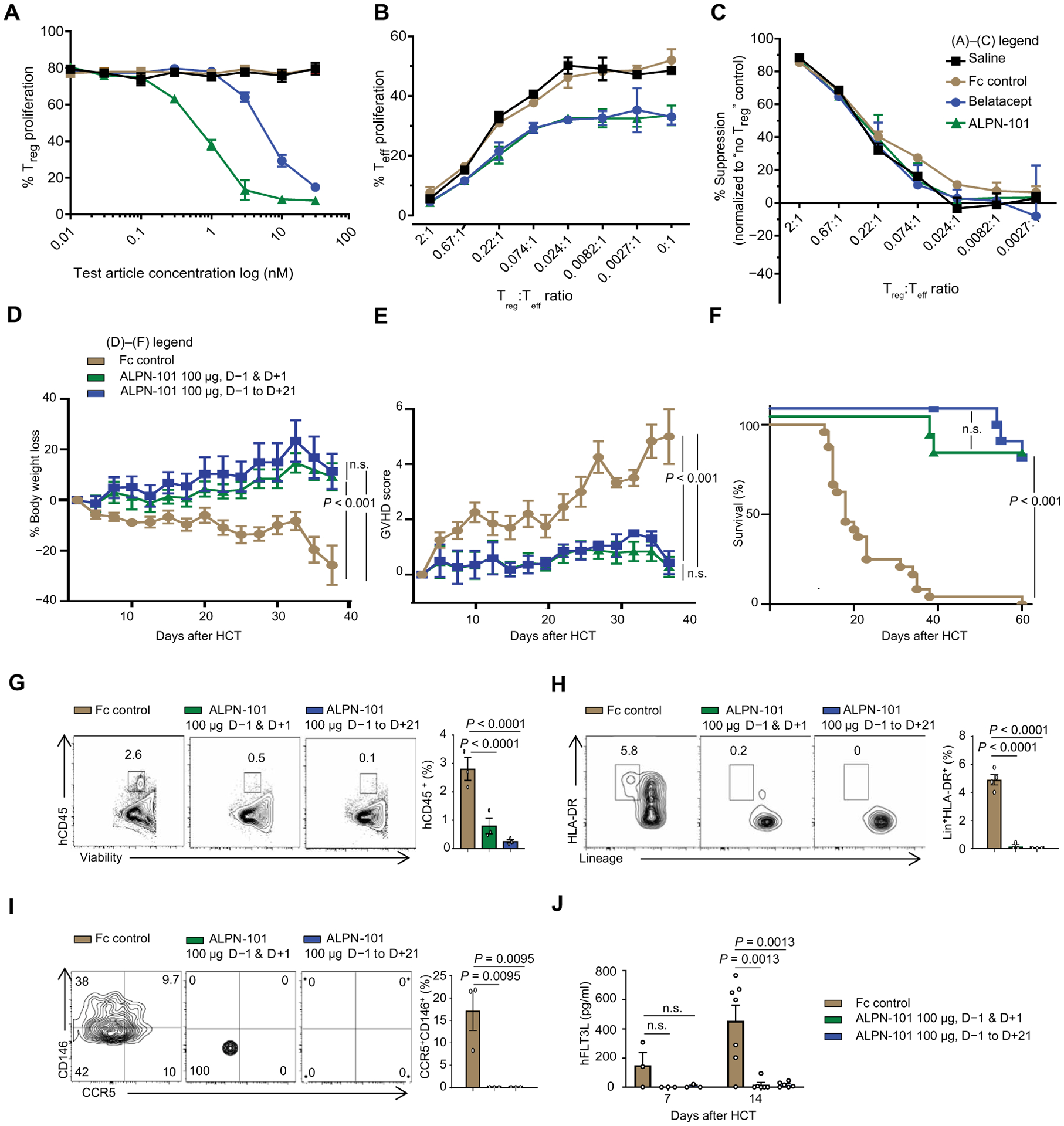
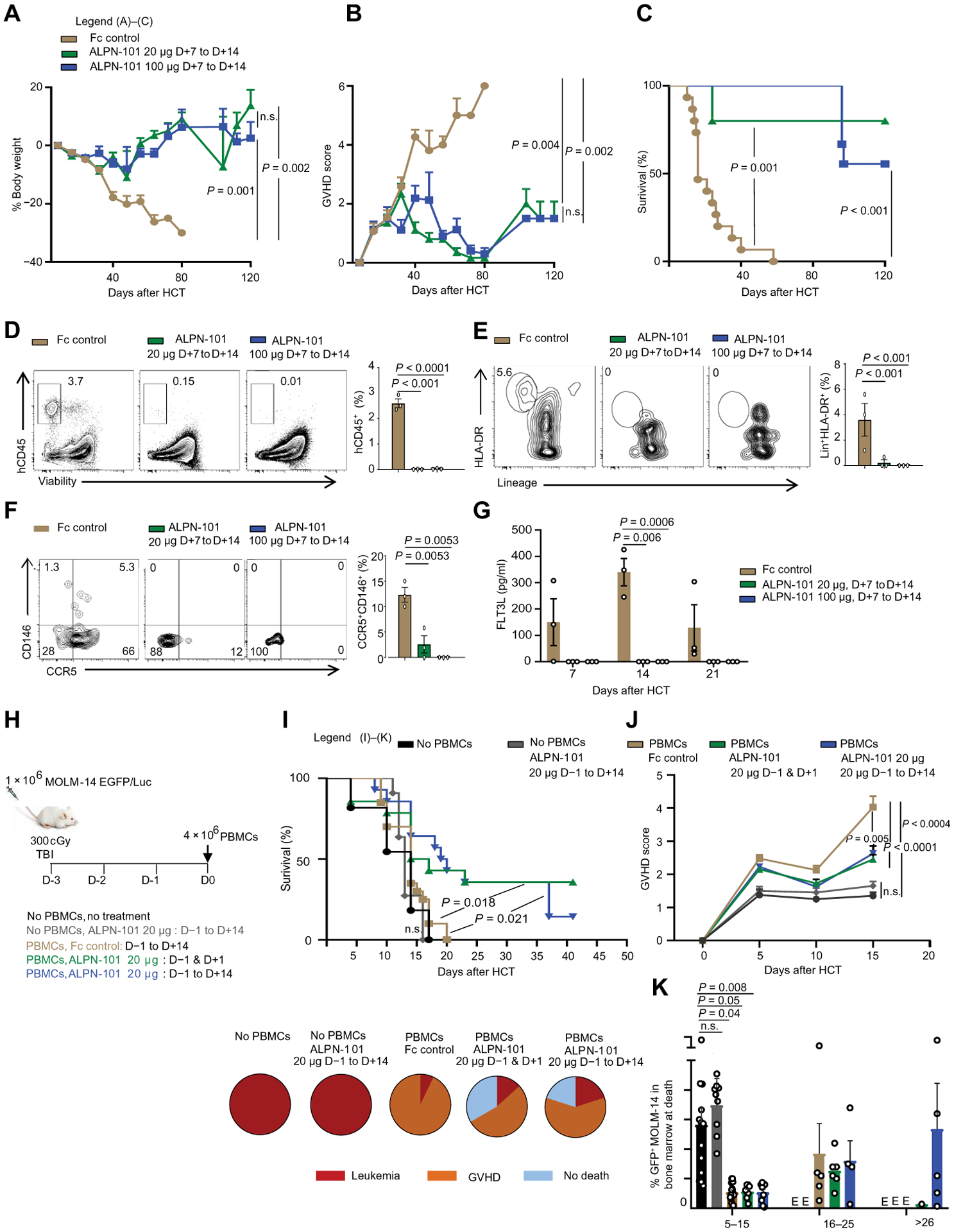
Acute graft-versus-host disease (aGVHD) remains a major complication of allogeneic hematopoietic cell transplantation (HCT). CD146 and CCR5 are proteins that mark activated T helper 17 (Th17) cells. The Th17 cell phenotype is promoted by the interaction of the receptor ICOS on T cells with ICOS ligand (ICOSL) on dendritic cells (DCs). We performed multiparametric flow cytometry in a cohort of 156 HCT recipients and conducted experiments with aGVHD murine models to understand the role of ICOSL+ DCs. We observed an increased frequency of ICOSL+ plasmacytoid DCs, correlating with CD146+CCR5+ T cell frequencies, in the 64 HCT recipients with gastrointestinal aGVHD. In murine models, donor bone marrow cells from ICOSL-deficient mice compared to those from wild-type mice reduced aGVHD-related mortality. Reduced aGVHD resulted from lower intestinal infiltration of pDCs and pathogenic Th17 cells. We transplanted activated human ICOSL+ pDCs along with human peripheral blood mononuclear cells into immunocompromised mice and observed infiltration of intestinal CD146+CCR5+ T cells. We found that prophylactic administration of a dual human ICOS/CD28 antagonist (ALPN-101) prevented aGVHD in this model better than did the clinically approved belatacept (CTLA-4-Fc), which binds CD80 (B7-1) and CD86 (B7-2) and interferes with the CD28 T cell costimulatory pathway. When started at onset of aGVHD signs, ALPN-101 treatment alleviated symptoms of ongoing aGVHD and improved survival while preserving antitumoral cytotoxicity. Our data identified ICOSL+-pDCs as an aGVHD biomarker and suggest that coinhibition of the ICOSL/ICOS and B7/CD28 axes with one biologic drug may represent a therapeutic opportunity to prevent or treat aGVHD.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures
References
-
- Martin PJ, McDonald GB, Sanders JE, Anasetti C, Appelbaum FR, Deeg HJ, Nash RA, Petersdorf EW, Hansen JA, Storb R, Increasingly frequent diagnosis of acute gastrointestinal graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol. Blood Marrow Transplant 10, 320–327 (2004). - PubMed
-
- Vander Lugt MT, Braun TM, Hanash S, Ritz J, Ho VT, Antin JH, Zhang Q, Wong CH, Wang H, Chin A, Gomez A, Harris AC, Levine JE, Choi SW, Couriel D, Reddy P, Ferrara JL, Paczesny S, ST2 as a marker for risk of therapy-resistant graft-versus-host disease and death. N. Engl. J. Med 369, 529–539 (2013). - PMC - PubMed
-
- Hartwell MJ, Ozbek U, Holler E, Renteria AS, Major-Monfried H, Reddy P, Aziz M, Hogan WJ, Ayuk F, Efebera YA, Hexner EO, Bunworasate U, Qayed M, Ordemann R, Wolfl M, Mielke S, Pawarode A, Chen YB, Devine S, Harris AC, Jagasia M, Kitko CL, Litzow MR, Kroger N, Locatelli F, Morales G, Nakamura R, Reshef R, Rosler W, Weber D, Wudhikarn K, Yanik GA, Levine JE, Ferrara JL, An early-biomarker algorithm predicts lethal graft-versus-host disease and survival. JCI Insight 2, e89798 (2017). - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
