

Deep learning in glaucoma with optical coherence tomography: a review
- PMID: 33028972
- PMCID: PMC7852526
- DOI: 10.1038/s41433-020-01191-5
Deep learning in glaucoma with optical coherence tomography: a review
Erratum in
-
Correction: Deep learning in glaucoma with optical coherence tomography: a review.Eye (Lond). 2021 Jan;35(1):357. doi: 10.1038/s41433-020-01244-9. Eye (Lond). 2021. PMID: 33097920 Free PMC article. No abstract available.
Abstract
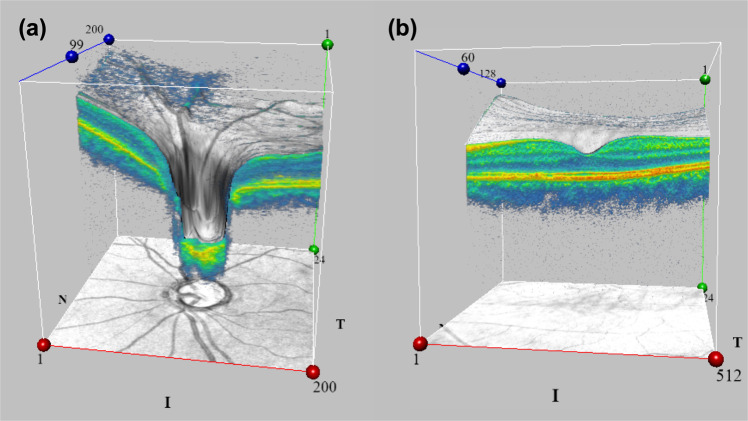
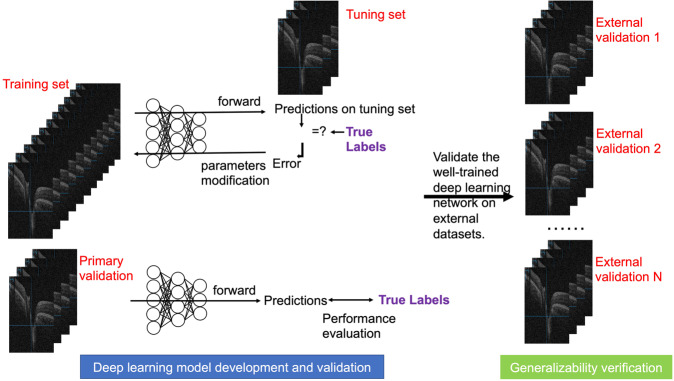
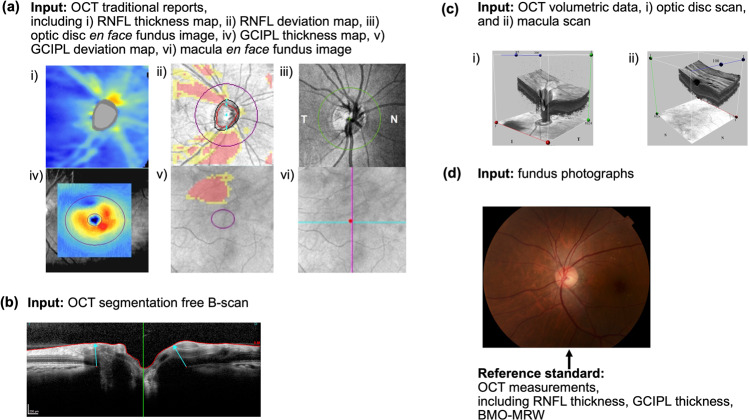
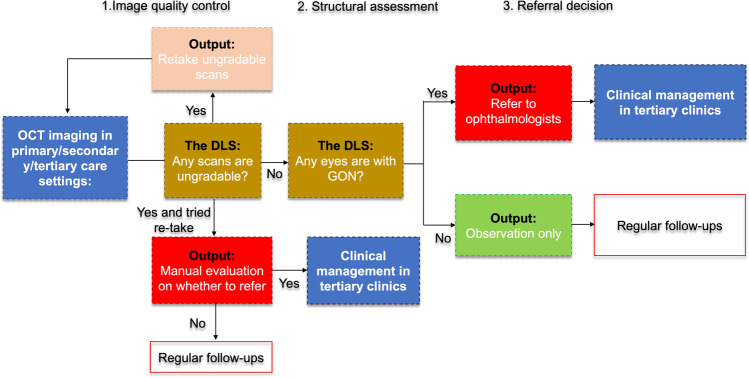
Deep learning (DL), a subset of artificial intelligence (AI) based on deep neural networks, has made significant breakthroughs in medical imaging, particularly for image classification and pattern recognition. In ophthalmology, applying DL for glaucoma assessment with optical coherence tomography (OCT), including OCT traditional reports, two-dimensional (2D) B-scans, and three-dimensional (3D) volumetric scans, has increasingly raised research interests. Studies have demonstrated that using DL for interpreting OCT is efficient, accurate, and with good performance for discriminating glaucomatous eyes from normal eyes, suggesting that incorporation of DL technology in OCT for glaucoma assessment could potentially address some gaps in the current practice and clinical workflow. However, further research is crucial in tackling some existing challenges, such as annotation standardization (i.e., setting a standard for ground truth labelling among different studies), development of DL-powered IT infrastructure for real-world implementation, prospective validation in unseen datasets for further evaluation of generalizability, cost-effectiveness analysis after integration of DL, the AI "black box" explanation problem. This review summarizes recent studies on the application of DL on OCT for glaucoma assessment, identifies the potential clinical impact arising from the development and deployment of the DL models, and discusses future research directions.
摘要: 深度学习 (DL) 作为基于深层神经网络的人工智能 (AI) 的一个子集, 在医学成像领域, 特别是图像分类和模式识别方面, 已取得重大突破。在眼科领域, 将DL应用于光学相干断层扫描 (OCT), 包括传统的OCT报告、二维B扫描和三维立体扫描, 从而对青光眼进行评估已引发了越来越多的研究兴趣。研究表明, 应用DL对 OCT的结果进行解读是有效、准确的, 并且能很好地区分青光眼和正常眼, 这表明DL技术与OCT结合对青光眼进行评估可弥补当前实践和临床流程中的一些空白。然而, 对于一些现存的挑战, 进一步研究是至关重要的, 例如注释标准化 (即在不同的研究中设定基础事实标签的标准), 为实际应用开发基于DL支持的IT基础架构, 在不可见的数据集中进行前瞻性验证以进一步评估泛化能力, 整合DL后的成本效益分析, 以及AI“黑箱”问题解释。本综述总结了应用DL在OCT评估青光眼的最新研究进展, 确定DL模型的开发和部署所带来的潜在临床影响, 并对未来的研究方向进行了讨论。.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Nicoara S. The mechanisms of neuronal death in glaucoma. Oftalmologia. 2000;51:4–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
