

Edema-like marrow signal intensity: a narrative review with a pictorial essay
- PMID: 33029648
- PMCID: PMC7875957
- DOI: 10.1007/s00256-020-03632-4
Edema-like marrow signal intensity: a narrative review with a pictorial essay
Abstract
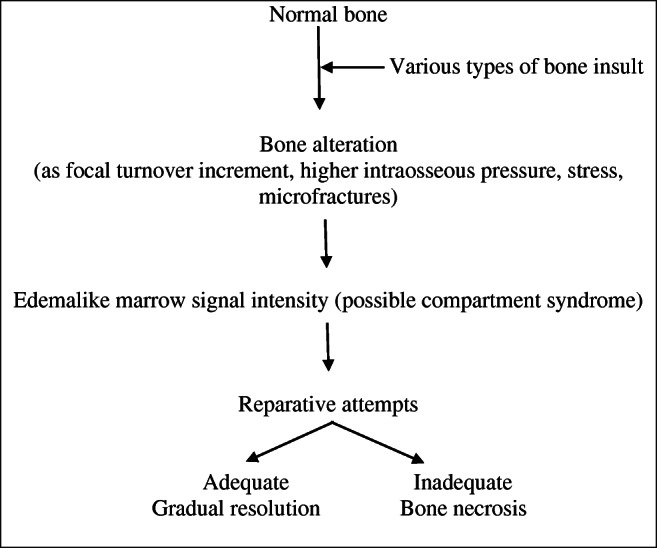
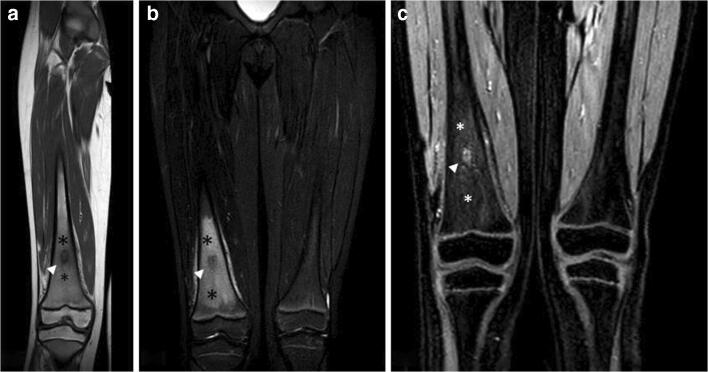
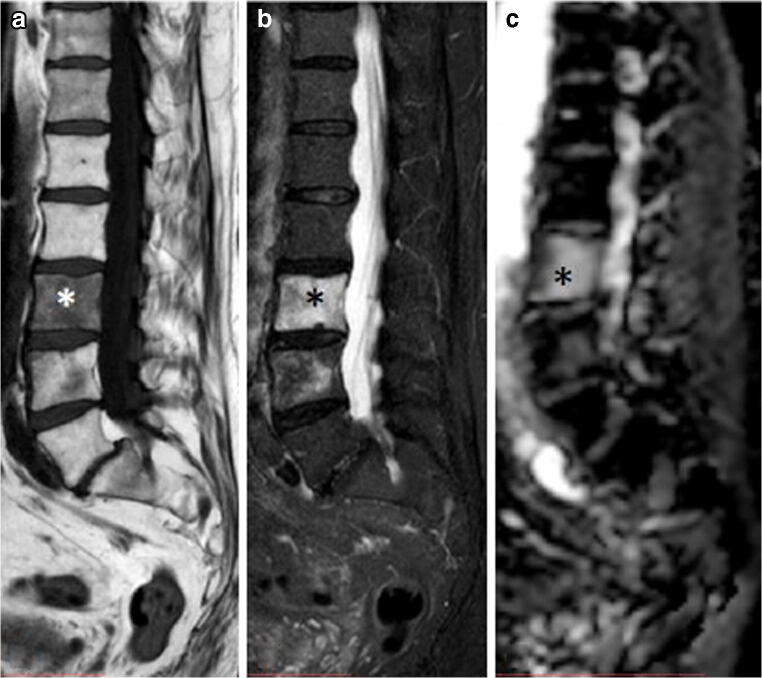
The term edema-like marrow signal intensity (ELMSI) represents a general term describing an area of abnormal signal intensity at MRI. Its appearance includes absence of clear margins and the possibility of exceeding well-defined anatomical borders (for example, physeal scars). We can define "ELMSI with unknown cause" an entity where the characteristic MR appearance is associated with the absence of specific signs of an underlying condition. However, it is more often an important finding indicating the presence of an underlying disease, and we describe this case as "ELMSI with known cause." It presents a dynamic behavior and its evolution can largely vary. It initially corresponds to an acute inflammatory response with edema, before being variably replaced by more permanent marrow remodeling changes such as fibrosis or myxomatous connective tissue that can occur over time. It is important to study ELMSI variations over time in order to evaluate the activity state and therapeutic response of an inflammatory chronic joint disease, the resolution of a trauma, and the severity of an osteoarthritis. We propose a narrative review of the literature dealing with various subjects about this challenging topic that is imaging, temporal evolution, etiology, differential diagnoses, and possible organization, together with a pictorial essay.
Keywords: AVN; Edema-like marrow signal intensity; MRI; Rheumatoid arthritis; SIFK.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures




Similar articles
-
Dual-energy CT virtual non-calcium: an accurate method for detection of knee osteoarthritis-related edema-like marrow signal intensity.Insights Imaging. 2023 Apr 30;14(1):74. doi: 10.1186/s13244-023-01407-8. Insights Imaging. 2023. PMID: 37121955 Free PMC article.
-
Edema-like marrow signal intensity (ELMSI) associated with nonossifying fibroma (NOF) on MRI: an uncommon finding in a common bone lesion.Skeletal Radiol. 2023 Aug;52(8):1511-1518. doi: 10.1007/s00256-023-04312-9. Epub 2023 Mar 3. Skeletal Radiol. 2023. PMID: 36867220
-
Bone marrow changes in osteoarthritis.Semin Musculoskelet Radiol. 2011 Jul;15(3):238-46. doi: 10.1055/s-0031-1278423. Epub 2011 Jun 3. Semin Musculoskelet Radiol. 2011. PMID: 21644197 Review.
-
Magnetic resonance imaging of subchondral bone marrow lesions in association with osteoarthritis.Semin Arthritis Rheum. 2012 Oct;42(2):105-18. doi: 10.1016/j.semarthrit.2012.03.009. Epub 2012 Apr 26. Semin Arthritis Rheum. 2012. PMID: 22542276 Free PMC article. Review.
-
[Research progress of bone marrow edema-like lesions in knee osteoarthritis].Zhongguo Gu Shang. 2021 Dec 25;34(12):1186-90. doi: 10.12200/j.issn.1003-0034.2021.12.018. Zhongguo Gu Shang. 2021. PMID: 34965640 Review. Chinese.
Cited by
-
Sacroiliac Bone Marrow Edema: Innocent Until Proven Guilty?Arthritis Rheumatol. 2022 Sep;74(9):1474-1476. doi: 10.1002/art.42143. Epub 2022 Aug 9. Arthritis Rheumatol. 2022. PMID: 35436388 Free PMC article. No abstract available.
-
MRI in axial spondyloarthritis: understanding an 'ASAS-positive MRI' and the ASAS classification criteria.Skeletal Radiol. 2022 Sep;51(9):1721-1730. doi: 10.1007/s00256-022-04018-4. Epub 2022 Feb 23. Skeletal Radiol. 2022. PMID: 35199195 Free PMC article. Review.
-
Dual-energy CT virtual non-calcium: an accurate method for detection of knee osteoarthritis-related edema-like marrow signal intensity.Insights Imaging. 2023 Apr 30;14(1):74. doi: 10.1186/s13244-023-01407-8. Insights Imaging. 2023. PMID: 37121955 Free PMC article.
-
MRI in the Diagnosis and Treatment Response Assessment of Chronic Nonbacterial Osteomyelitis in Children and Adolescents.Curr Rheumatol Rep. 2022 Feb;24(2):27-39. doi: 10.1007/s11926-022-01053-x. Epub 2022 Feb 8. Curr Rheumatol Rep. 2022. PMID: 35133566 Review.
-
Pictorial review: challenges in distinguishing bilateral metaphyseal marrow abnormalities on magnetic resonance imaging.Pediatr Radiol. 2024 Jul;54(8):1247-1260. doi: 10.1007/s00247-024-05896-7. Epub 2024 Mar 16. Pediatr Radiol. 2024. PMID: 38491225 Review.
References
-
- Gorbachova T, Amber I, Beckmann NM, Bennett DL, Chang EY, Davis L, et al. Nomenclature of subchondral nonneoplastic bone lesions. Am J Roentgenol. 2019:1–20. 10.2214/ajr.19.21571. - PubMed
-
- Solomon L. Bone-marrow oedema syndrome. J Bone Joint Surg. 1993;75B:175–176. - PubMed
-
- Thiryayi WA, Thiryayi SA, Freemont AJ. Histopathological perspective on bone marrow oedema reactive bone change and haemorrhage. Eur J Radiol. 2008;67:62–67. - PubMed
-
- Lang P, Genant HK, Majumadar S. In: Bone marrow disorders. MRI of the musculoskeletal system. Chan WP, Lang P, Genant HK, editors. Philadelphia: WB Saunders; 1994. pp. 445–485.
-
- Vogler JB, III, Murphy WA., Jr . In: Diffuse marrow diseases. MRI of the musculoskeletal system. Berquest TH, editor. Philadelphia: Lippincott, Williams & Wilkins; 2001. pp. 979–1028.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
