

Clinical and microbiological characteristics of adults with hospital-acquired pneumonia: a 10-year prospective observational study in China
- PMID: 33029764
- PMCID: PMC7540435
- DOI: 10.1007/s10096-020-04046-9
Clinical and microbiological characteristics of adults with hospital-acquired pneumonia: a 10-year prospective observational study in China
Abstract
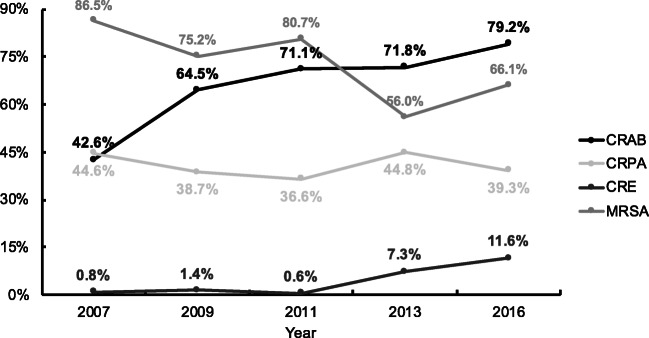
Hospital-acquired pneumonia (HAP) is a significant nosocomial infection; data on the distribution and antimicrobial resistance profiles of HAP in China are limited. We included 2827 adult patients with HAP from the Chinese Antimicrobial Resistance Surveillance of Nosocomial Infections network admitted in 15 Chinese teaching hospitals between 2007 and 2016. Clinical data and antimicrobial susceptibility of isolated pathogens were obtained from the medical records and central laboratory, respectively. Multivariable logistic regression was performed to determine the risk factors for mortality and multidrug resistance (MDR). A total of 386 (13.7%) patients died in the hospital, while 1181 (41.8%) developed ventilator-associated pneumonia (VAP). Active immunosuppressant therapy (OR 1.915 (95% CI 1.475-2.487)), solid tumor (OR 1.860 (95% CI 1.410-2.452)), coma (OR 1.783 (95% CI 1.364-2.333)), clinical pulmonary infection score ≥7 (OR 1.743 (95% CI 1.373-2.212)), intensive care unit stay (OR 1.652 (95% CI 1.292-2.111)), age ≥65 years (OR 1.621 (95% CI 1.282-2.049)), and tracheal cannula insertion (OR 1.613 (95% CI 1.169-2.224)) were independent risk factors for in-hospital mortality. Liver cirrhosis (OR 3.120 (95% CI 1.436-6.780)) and six other variables were independent predictors of MDR. Acinetobacter baumannii (25.6%), Pseudomonas aeruginosa (20.1%), Klebsiella pneumoniae (15.4%), and Staphylococcus aureus (12.6%) were the most common pathogens (MDR prevalence 64.9%). Isolates from VAP patients showed more A. baumannii and less K. pneumoniae and E. coli strains (p < 0.001, respectively) than those from patients without VAP. The proportion of methicillin-resistant S. aureus strains decreased; that of carbapenem-resistant A. baumannii and Enterobacterales strains increased. There had been changes in the antibiotic resistance profiles of HAP pathogens in China. Risk factors for mortality and MDR are important for the selection of antimicrobials for HAP in China.
Keywords: Antimicrobial resistance; Hospital-acquired pneumonia; Mortality; Multidrug resistance; Risk factor.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Torres A, Niederman MS, Chastre J, Ewig S, Fernandez-Vandellos P, Hanberger H, Kollef M, Li Bassi G, Luna CM, Martin-Loeches I, Paiva JA, Read RC, Rigau D, Timsit JF, Welte T, Wunderink R (2017) International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J 50(3). 10.1183/13993003.00582-2017 - PubMed
-
- Chung DR, Song JH, Kim SH, Thamlikitkul V, Huang SG, Wang H, So TM, Yasin RM, Hsueh PR, Carlos CC, Hsu LY, Buntaran L, Lalitha MK, Kim MJ, Choi JY, Kim SI, Ko KS, Kang CI, Peck KR. High prevalence of multidrug-resistant nonfermenters in hospital-acquired pneumonia in Asia. Am J Respir Crit Care Med. 2011;184(12):1409–1417. doi: 10.1164/rccm.201102-0349OC. - DOI - PubMed
-
- Kalil AC, Metersky ML, Klompas M, Muscedere J, Sweeney DA, Palmer LB, Napolitano LM, O'Grady NP, Bartlett JG, Carratala J, El Solh AA, Ewig S, Fey PD, File TM, Jr, Restrepo MI, Roberts JA, Waterer GW, Cruse P, Knight SL, Brozek JL. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;63(5):e61–e111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
