

Depression Is Associated With Preserved Cortical Thickness Relative to Apathy in Frontotemporal Dementia
- PMID: 33030106
- PMCID: PMC8026775
- DOI: 10.1177/0891988720964258
Depression Is Associated With Preserved Cortical Thickness Relative to Apathy in Frontotemporal Dementia
Abstract
Objectives: To understand the differential neuroanatomical substrates underlying apathy and depression in Frontotemporal dementia (FTD).
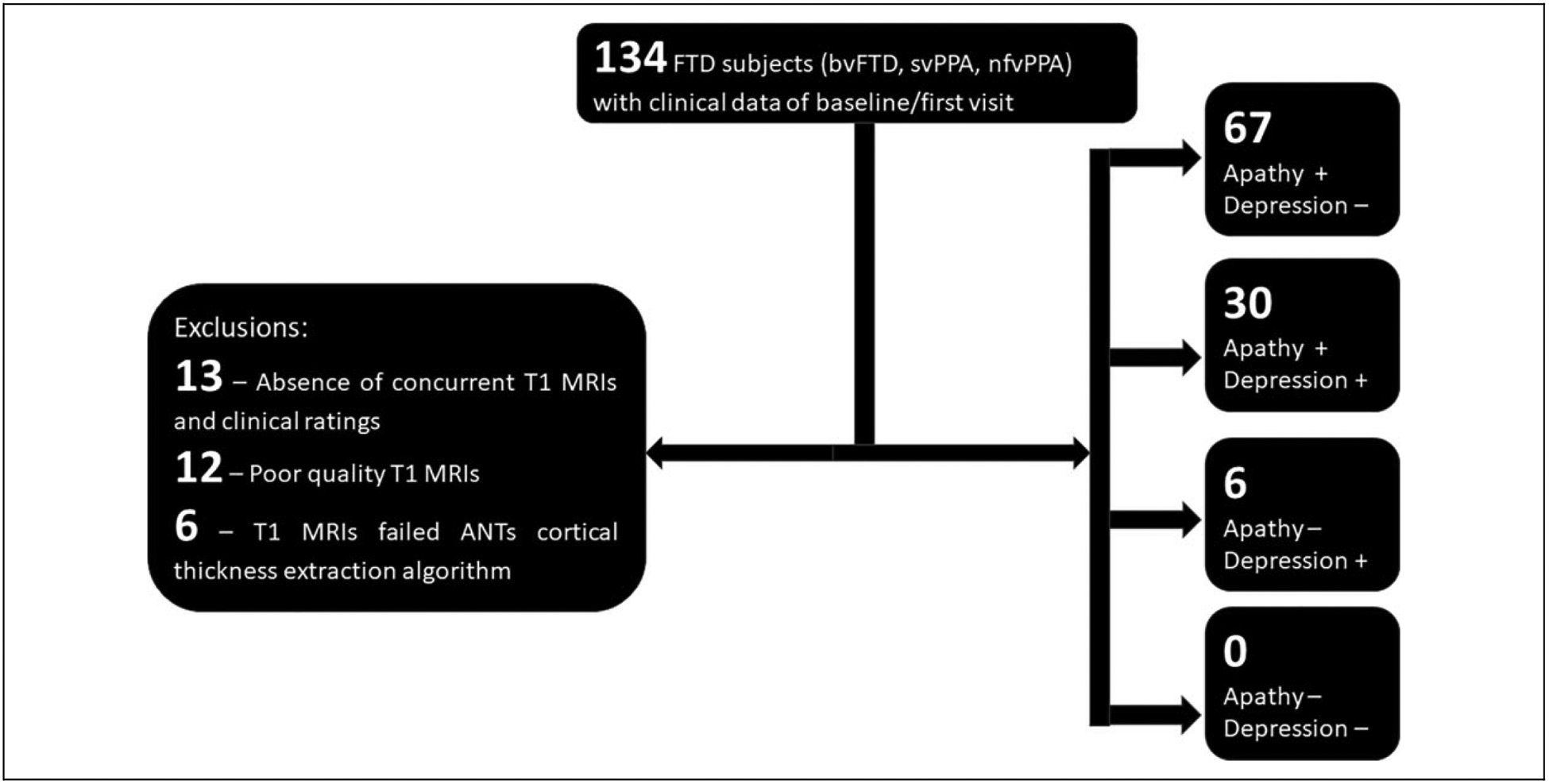
Methods: T1-MRIs and clinical data of patients with behavioral and aphasic variants of FTD were obtained from an open database. Cortical thickness was derived, its association with apathy severity and difference between the depressed and not depressed were examined with appropriate covariates.
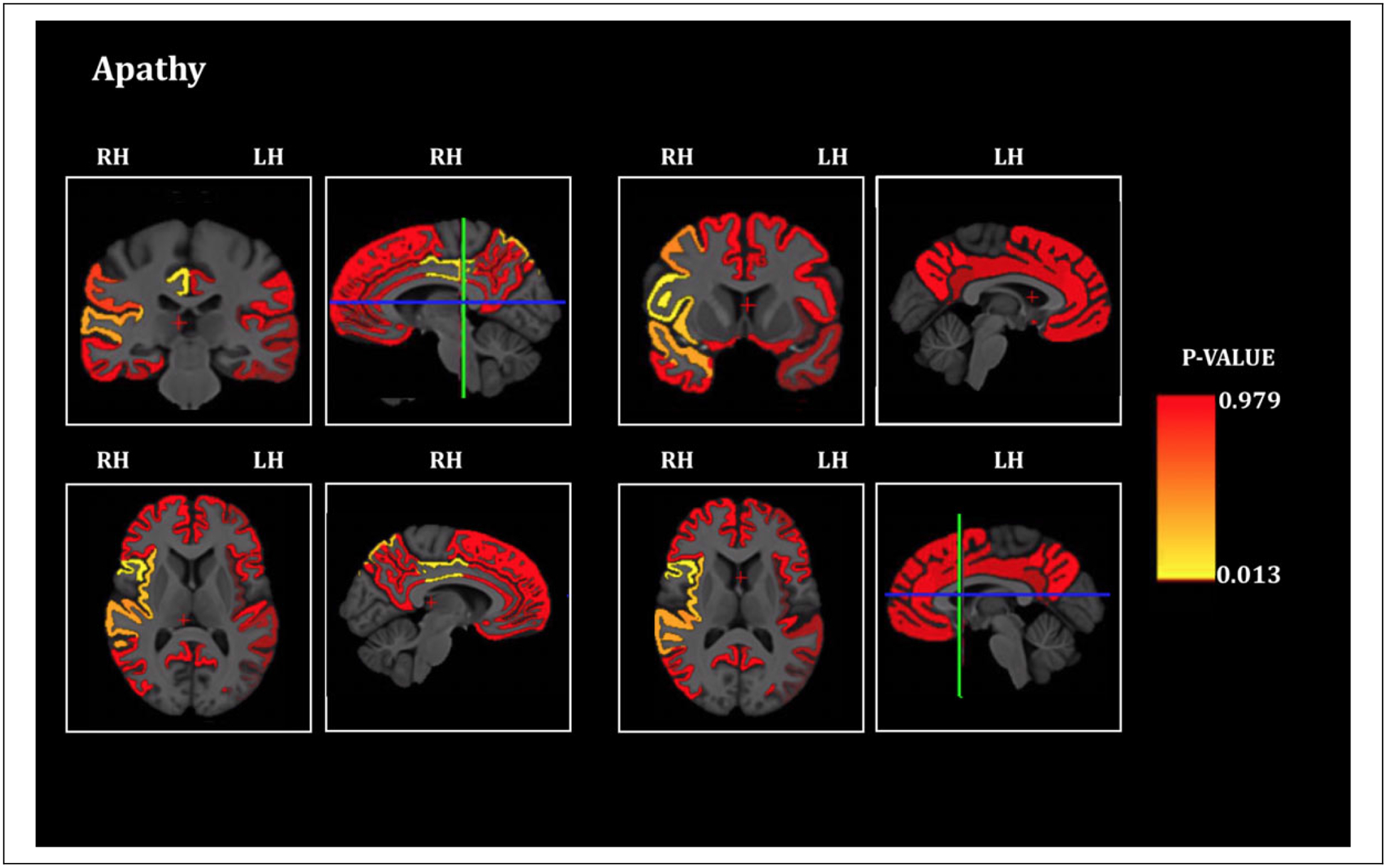
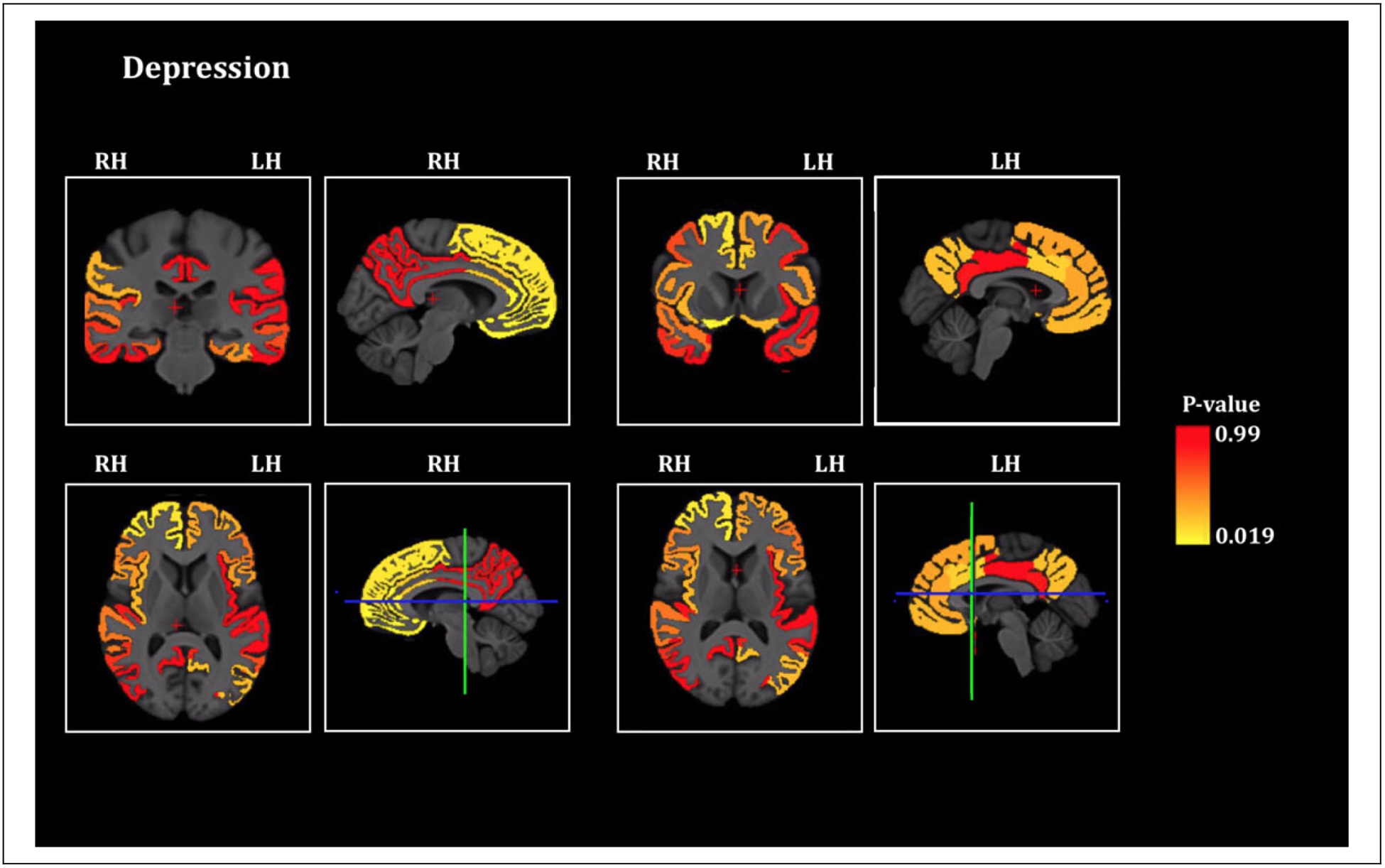
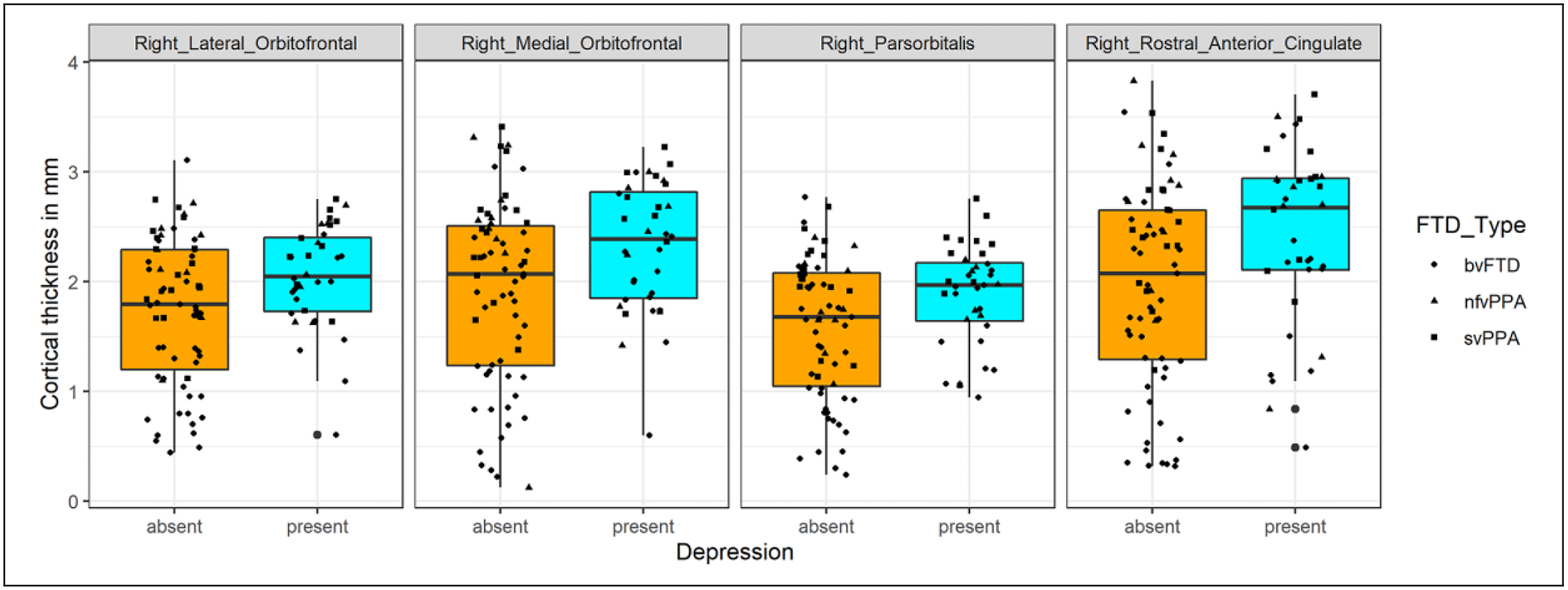
Results: Apathy severity was significantly associated with cortical thinning of the lateral parts of the right sided frontal, temporal and parietal lobes. The right sided orbitofrontal, parsorbitalis and rostral anterior cingulate cortex were thicker in depressed compared to patients not depressed.
Conclusions: Greater thickness of right sided ventromedial and inferior frontal cortex in depression compared to patients without depression suggests a possible requisite of gray matter in this particular area for the manifestation of depression in FTD. This study demonstrates a method for deriving neuroanatomical patterns across non-harmonized neuroimaging data in a neurodegenerative disease.
Keywords: apathy; cortical thickness; depression; frontotemporal dementia; right frontal cortex; structural MRI.
Conflict of interest statement
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Dr. Rakshathi Basavaraju reports no disclosures. Dr. Xinyang Feng is currently a Research Scientist at Facebook Inc. He participated in this study when he was a PhD student in the Department of Biomedical Engineering, Columbia University. Ms. Jeanelle France reports no disclosures. Dr. Edward D. Huey reports no disclosures. Dr. Frank A. Provenzano is a consultant for and has equity in IMIJ technologies.
Figures
Similar articles
-
Cortical signature of depressive symptoms in frontotemporal dementia: A surface-based analysis.Ann Clin Transl Neurol. 2023 Oct;10(10):1704-1713. doi: 10.1002/acn3.51860. Epub 2023 Jul 31. Ann Clin Transl Neurol. 2023. PMID: 37522381 Free PMC article.
-
Differences of apathy perfusion correlates between Alzheimer's disease and frontotemporal dementia. A 99mTc-HMPAO SPECT study with automated Brodmann areas analysis.Int J Psychiatry Clin Pract. 2022 Mar;26(1):14-22. doi: 10.1080/13651501.2020.1846752. Epub 2020 Nov 18. Int J Psychiatry Clin Pract. 2022. PMID: 33207961
-
Apathy: a neurocircuitry model based on frontotemporal dementia.J Neurol Neurosurg Psychiatry. 2018 Apr;89(4):389-396. doi: 10.1136/jnnp-2017-316277. Epub 2017 Oct 24. J Neurol Neurosurg Psychiatry. 2018. PMID: 29066518 Free PMC article. Review.
-
Brain Regions Involved in Arousal and Reward Processing are Associated with Apathy in Alzheimer's Disease and Frontotemporal Dementia.J Alzheimers Dis. 2017;55(2):551-558. doi: 10.3233/JAD-160107. J Alzheimers Dis. 2017. PMID: 27802220
-
Neural correlates of apathy in patients with neurodegenerative disorders: an activation likelihood estimation (ALE) meta-analysis.Brain Imaging Behav. 2019 Dec;13(6):1815-1834. doi: 10.1007/s11682-018-9959-0. Brain Imaging Behav. 2019. PMID: 30238208 Review.
Cited by
-
The importance of a multidimensional approach to the preclinical study of major depressive disorder and apathy.Emerg Top Life Sci. 2022 Dec 9;6(5):479-489. doi: 10.1042/ETLS20220004. Emerg Top Life Sci. 2022. PMID: 36413089 Free PMC article.
-
Behavioural changes in frontotemporal dementia and their cognitive and neuroanatomical correlates.Brain. 2025 Aug 1;148(8):2730-2745. doi: 10.1093/brain/awaf061. Brain. 2025. PMID: 39938002 Free PMC article.
-
A transdiagnostic review of neuroimaging studies of apathy and disinhibition in dementia.Brain. 2022 Jun 30;145(6):1886-1905. doi: 10.1093/brain/awac133. Brain. 2022. PMID: 35388419 Free PMC article. Review.
-
Cortical signature of depressive symptoms in frontotemporal dementia: A surface-based analysis.Ann Clin Transl Neurol. 2023 Oct;10(10):1704-1713. doi: 10.1002/acn3.51860. Epub 2023 Jul 31. Ann Clin Transl Neurol. 2023. PMID: 37522381 Free PMC article.
-
Advances in the study of apathy related to cerebral small vessel disease.Front Neurol. 2025 Feb 12;16:1513574. doi: 10.3389/fneur.2025.1513574. eCollection 2025. Front Neurol. 2025. PMID: 40013000 Free PMC article. Review.
References
-
- Hogan DB, Jette N, Fiest KM, et al. The prevalence and incidence of frontotemporal dementia: a systematic review. Can J Neurol Sci. 2016;43(Suppl 1):S96–S109. - PubMed
-
- Galimberti D, Dell’Osso B, Altamura AC, Scarpini E. Psychiatric symptoms in frontotemporal dementia: epidemiology, phenotypes, and differential diagnosis. Biol Psychiatry. 2015;78(10): 684–692. - PubMed
-
- Levy R, Dubois B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cereb Cortex. 2006; 16(7):916–928. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
