

Physiologically-Based Pharmacokinetic Modeling for the Prediction of a Drug-Drug Interaction of Combined Effects on P-glycoprotein and Cytochrome P450 3A
- PMID: 33030266
- PMCID: PMC7679072
- DOI: 10.1002/psp4.12562
Physiologically-Based Pharmacokinetic Modeling for the Prediction of a Drug-Drug Interaction of Combined Effects on P-glycoprotein and Cytochrome P450 3A
Abstract
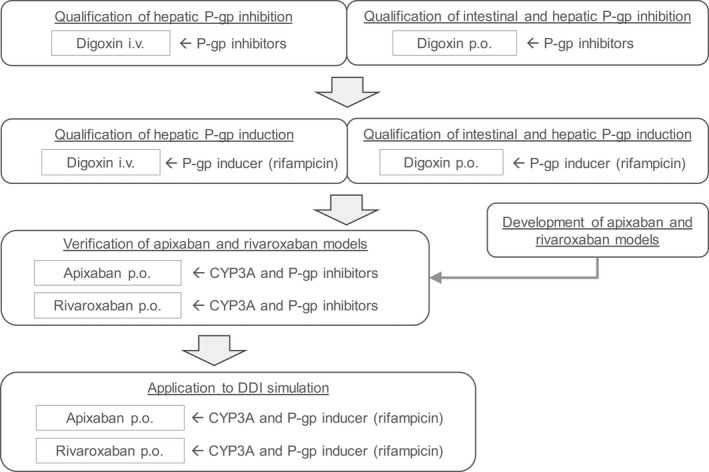
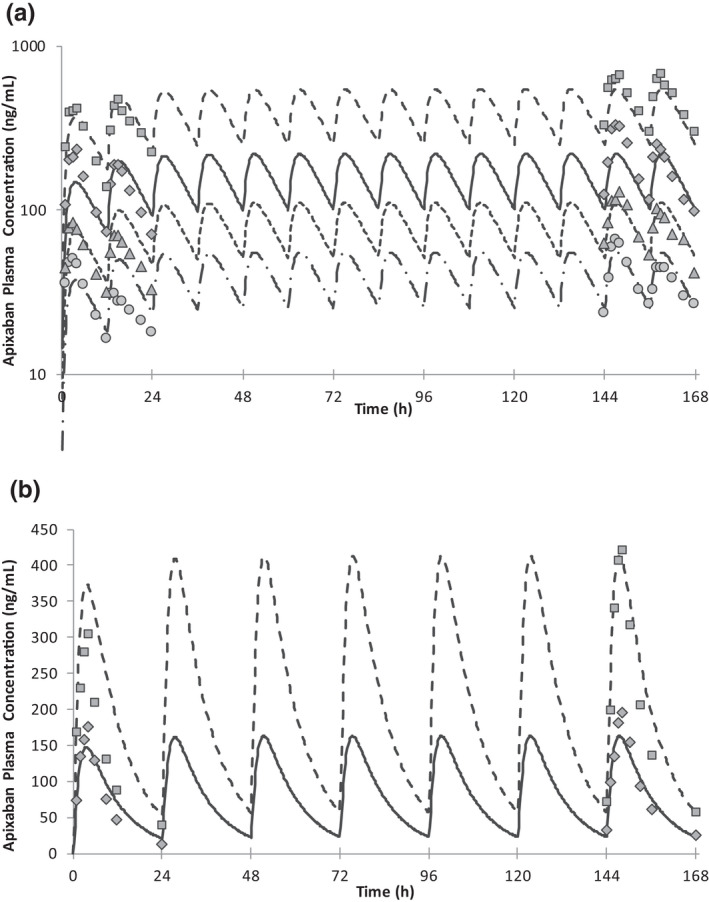
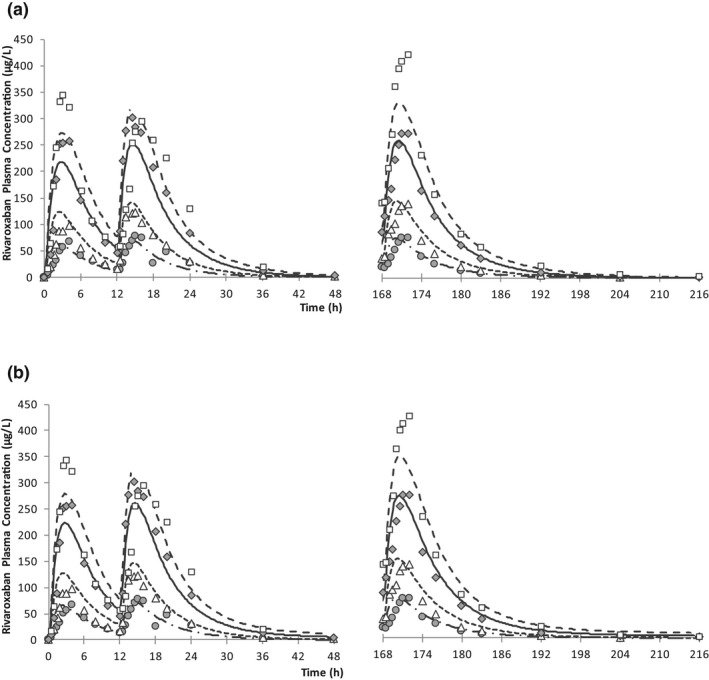
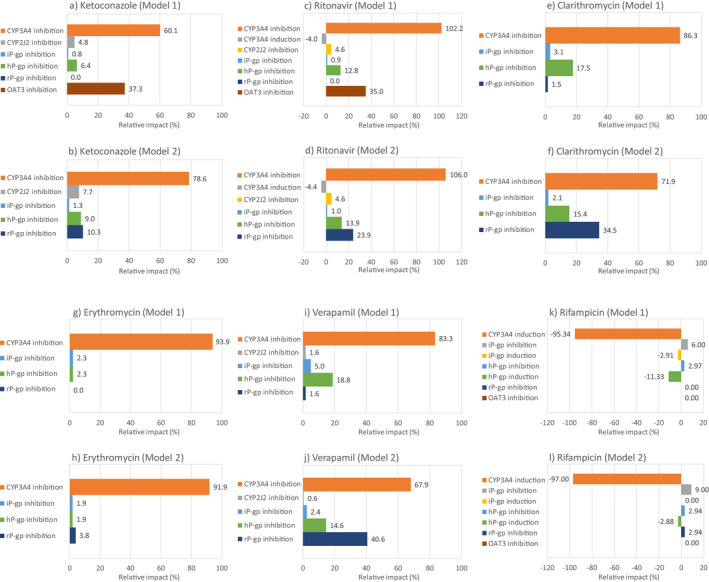
Direct oral anticoagulants, such as apixaban and rivaroxaban, are important for the treatment and prophylaxis of venous thromboembolism and to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation. Because apixaban and rivaroxaban are predominantly eliminated by cytochrome P450 (CYP) 3A and P-glycoprotein (P-gp), concomitant use of combined P-gp and strong CYP3A4 inhibitors and inducers should be avoided. Physiologically-based pharmacokinetic models for apixaban and rivaroxaban were developed to estimate the net effect of CYP3A induction, P-gp inhibition, and P-gp induction by rifampicin. The disposition of rivaroxaban is more complex compared with apixaban because both hepatic and renal P-gp is considered to contribute to rivaroxaban elimination. Furthermore, organic anion transporter-3, a renal uptake transporter, may also contribute the elimination of rivaroxaban from systemic circulation. The models were verified with observed clinical drug-drug interactions with CYP3A and P-gp inhibitors. With the developed models, the predicted area under the concentration time curve and maximum concentration ratios were 0.43 and 0.48, respectively, for apixaban, and 0.50-0.52 and 0.72-0.73, respectively, for rivaroxaban when coadministered with 600 mg multiple doses of rifampicin and that were very close to observed data. The impact of each of the elimination pathways was assessed for rivaroxaban, and inhibition of CYP3A led to a larger impact over intestinal and hepatic P-gp. Inhibition of renal organic anion transporter-3 or P-gp led to an overall modest interaction. The developed apixaban and rivaroxaban models can be further applied to the investigation of interactions with other P-gp and/or CYP3A4 inhibitors and inducers.
© 2020 Astellas Pharma Inc. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals LLC on behalf of the American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no competing interests for this work.
Figures
Similar articles
-
Predicting drug-drug interactions with physiologically based pharmacokinetic/pharmacodynamic modelling and optimal dosing of apixaban and rivaroxaban with dronedarone co-administration.Thromb Res. 2022 Oct;218:24-34. doi: 10.1016/j.thromres.2022.08.007. Epub 2022 Aug 11. Thromb Res. 2022. PMID: 35985100
-
Virtual twin approach using physiologically based pharmacokinetic modelling in hospitalized patients treated with apixaban or rivaroxaban.Br J Clin Pharmacol. 2025 Jul;91(7):2057-2069. doi: 10.1002/bcp.70032. Epub 2025 Mar 4. Br J Clin Pharmacol. 2025. PMID: 40035306
-
Effect of Clarithromycin, a Strong CYP3A and P-glycoprotein Inhibitor, on the Pharmacokinetics of Edoxaban in Healthy Volunteers and the Evaluation of the Drug Interaction with Other Oral Factor Xa Inhibitors by a Microdose Cocktail Approach.Cardiovasc Drugs Ther. 2024 Aug;38(4):747-756. doi: 10.1007/s10557-023-07443-2. Epub 2023 Mar 4. Cardiovasc Drugs Ther. 2024. PMID: 36870039 Free PMC article. Clinical Trial.
-
Pharmacokinetic and pharmacodynamic drug interactions with new oral anticoagulants: what do they mean for patients with atrial fibrillation?Ann Pharmacother. 2013 Nov;47(11):1478-87. doi: 10.1177/1060028013504741. Epub 2013 Oct 9. Ann Pharmacother. 2013. PMID: 24259602 Review.
-
Relevance of P-glycoprotein in stroke prevention with dabigatran, rivaroxaban, and apixaban.Herz. 2015 Apr;40 Suppl 2:140-5. doi: 10.1007/s00059-014-4188-9. Epub 2015 Jan 25. Herz. 2015. PMID: 25616425 Review.
Cited by
-
The Impact of Dexamethasone and Prednisone on Apixaban and Rivaroxaban Exposure in COVID-19 Patients: A Physiologically Based Pharmacokinetic Modeling Study.Clin Pharmacol Ther. 2025 Feb;117(2):554-560. doi: 10.1002/cpt.3491. Epub 2024 Nov 13. Clin Pharmacol Ther. 2025. PMID: 39535447 Free PMC article.
-
Physiologically based pharmacokinetic modeling of apixaban to predict exposure in populations with hepatic and renal impairment and elderly populations.Eur J Clin Pharmacol. 2024 Feb;80(2):261-271. doi: 10.1007/s00228-023-03602-4. Epub 2023 Dec 15. Eur J Clin Pharmacol. 2024. PMID: 38099940 Free PMC article.
-
Physiologically-based pharmacokinetic modeling to evaluate in vitro-to-in vivo extrapolation for intestinal P-glycoprotein inhibition.CPT Pharmacometrics Syst Pharmacol. 2022 Jan;11(1):55-67. doi: 10.1002/psp4.12733. Epub 2021 Nov 6. CPT Pharmacometrics Syst Pharmacol. 2022. PMID: 34668334 Free PMC article.
-
Physiologically-based pharmacokinetic modeling to predict drug-drug interactions of dabigatran etexilate and rivaroxaban in the Chinese older adults.Eur J Pharm Sci. 2023 Mar 1;182:106376. doi: 10.1016/j.ejps.2023.106376. Epub 2023 Jan 7. Eur J Pharm Sci. 2023. PMID: 36626944 Free PMC article.
-
Physiologically-based pharmacokinetic modeling to predict drug-drug interaction of enzalutamide with combined P-gp and CYP3A substrates.J Pharmacokinet Pharmacodyn. 2023 Oct;50(5):365-376. doi: 10.1007/s10928-023-09867-7. Epub 2023 Jun 21. J Pharmacokinet Pharmacodyn. 2023. PMID: 37344637 Free PMC article.
References
-
- Wagner, C. et al Predicting the effect of cytochrome P450 inhibitors on substrate drugs: analysis of physiologically based pharmacokinetic modeling submissions to the US Food and Drug Administration. Clin. Pharmacokinet. 54, 117–127 (2014). - PubMed
-
- Wagner, C. , Pan, Y. , Hsu, V. , Sinha, V. & Zhao, P. Predicting the effect of CYP3A inducers on the pharmacokinetics of substrate drugs using physiologically based pharmacokinetic (PBPK) modeling: an analysis of PBPK submissions to the US FDA. Clin. Pharmacokinet. 55, 475–483 (2015). - PubMed
-
- Rodrigues, A.D. , Lai, Y. , Shen, H. , Varma, M.V.S. , Rowland, A. & Oswald, S. Induction of human intestinal and hepatic organic anion transporting polypeptides: Where is the evidence for its relevance in drug‐drug interactions? Drug Metab. Dispos. 48, 205–216 (2020). - PubMed
-
- Pedersen, J.M. , Khan, E.K. , Bergström, C.A.S. , Palm, J. , Hoogstraate, J. & Artursson, P. Substrate and method dependent inhibition of three ABC‐transporters (MDR1, BCRP, and MRP2). Eur. J. Pharm. Sci. 103, 70–76 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
