

Retention-in-care in the PMTCT cascade: definitions matter! Analyses from the INSPIRE projects in Malawi, Nigeria and Zimbabwe
- PMID: 33030306
- PMCID: PMC7543052
- DOI: 10.1002/jia2.25609
Retention-in-care in the PMTCT cascade: definitions matter! Analyses from the INSPIRE projects in Malawi, Nigeria and Zimbabwe
Abstract
Introduction: Definitions of retention-in-care in Prevention of Mother-to-Child Transmission of HIV (PMTCT) vary substantially between studies and programmes. Some definitions are based on visits missed/made, others on a minimum total number of visits, or attendance at a final clinic visit at a specific time. An agreed definition could contribute to developing evidence-based interventions for improving retention-in-care. In this paper, we estimated retention-in-care rates according to different definitions, and we quantified and visualized the degree of agreement between definitions.
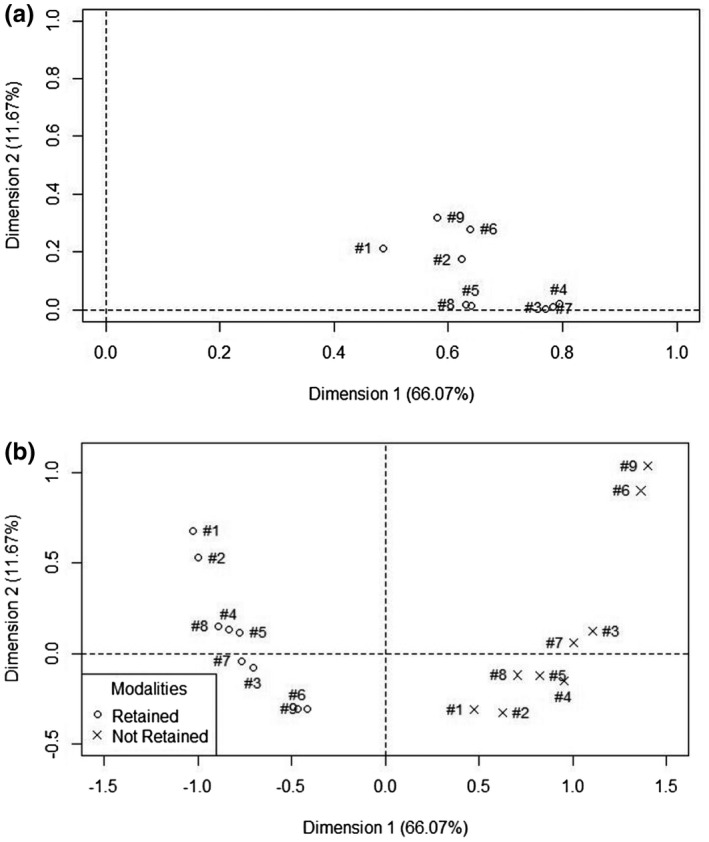
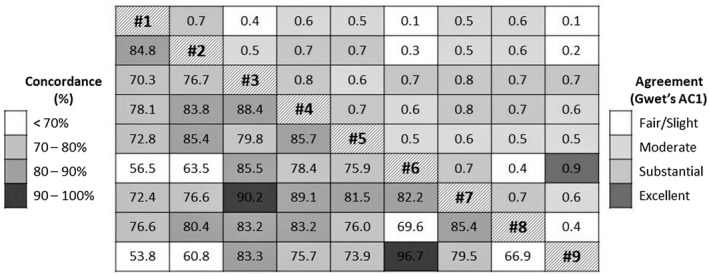
Methods: We calculated retention in care rates using nine definitions in the six INSPIRE PMTCT intervention studies, conducted in three sub-Saharan African countries between 2013 and 2017. With data from one of the studies (E4E), we estimated the agreement between definitions using Gwet's agreement coefficient (AC1) and concordance. We calculated positive predictive values (PPV) and negative predictive values (NPV) for all definitions considering successively each definition as the reference standard. Finally, we used a Multiple Correspondence Analysis (MCA) to examine clustering of the way different definitions handle retention-in-care.
Results: Retention-in-care rates among 5107 women ranged from 30% to 76% in the complete dataset with Gwet's AC1 being 0.56 [0.53; 0.59] indicating a moderate agreement between all definitions together. Two pairs of definitions with high inner concordance and agreement had either very high PPV or very high NPV, and appeared distinct from the other five definitions on the MCA figures. These pairs of definitions were also the ones resulting in the lowest and highest estimates of retention-in-care. The simplest definition, that only required a final clinic visit to classify women as retained in care, and classified 55% of women as retained in care, had a PPV ranging from 0.7 to 1 and a NPV ranging from 0.69 to 0.98 when excluding the two pairs afore-mentioned; it resulted in a moderate to substantial agreement and a 70% to 90% concordance with all other definitions.
Conclusions: Our study highlights the variability of definitions in estimating retention-in-care. Some definitions are very stringent which may be required in some instances. A simple indicator such as attendance at a single time point may be sufficient for programme planning and evaluation.
Keywords: Africa; HIV care continuum; PMTCT; outcome assessment; retention; women.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
Similar articles
-
Measuring retention in care for HIV-positive pregnant women in Prevention of Mother-to-Child Transmission of HIV (PMTCT) option B+ programs: the Mozambique experience.BMC Public Health. 2020 Mar 12;20(1):322. doi: 10.1186/s12889-020-8406-5. BMC Public Health. 2020. PMID: 32164601 Free PMC article.
-
The Roles of Expert Mothers Engaged in Prevention of Mother-to-Child Transmission (PMTCT) Programs: A Commentary on the INSPIRE Studies in Malawi, Nigeria, and Zimbabwe.J Acquir Immune Defic Syndr. 2017 Jun 1;75 Suppl 2:S224-S232. doi: 10.1097/QAI.0000000000001375. J Acquir Immune Defic Syndr. 2017. PMID: 28498193
-
Modeling the Impact of Retention Interventions on Mother-to-Child Transmission of HIV: Results From INSPIRE Studies in Malawi, Nigeria, and Zimbabwe.J Acquir Immune Defic Syndr. 2017 Jun 1;75 Suppl 2(2):S233-S239. doi: 10.1097/QAI.0000000000001364. J Acquir Immune Defic Syndr. 2017. PMID: 28498194 Free PMC article.
-
What interventions are effective in improving uptake and retention of HIV-positive pregnant and breastfeeding women and their infants in prevention of mother to child transmission care programmes in low-income and middle-income countries? A systematic review and meta-analysis.BMJ Open. 2019 Jul 29;9(7):e024907. doi: 10.1136/bmjopen-2018-024907. BMJ Open. 2019. PMID: 31362959 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
A qualitative study to understand the facilitators of and barriers to retention in care to the national PMTCT Option B+ programme in Uganda.PLoS One. 2025 Jan 16;20(1):e0314885. doi: 10.1371/journal.pone.0314885. eCollection 2025. PLoS One. 2025. PMID: 39820622 Free PMC article.
-
A Comparative Analysis of Different HIV Viral Load Suppression Definitions Among Clients Receiving Care in the Miami-Dade Ryan White HIV/AIDS Program.AIDS Behav. 2022 Nov;26(11):3576-3588. doi: 10.1007/s10461-022-03694-6. Epub 2022 May 10. AIDS Behav. 2022. PMID: 35536517 Free PMC article.
-
Disengagement from Care Among People Co-Infected with HIV and HCV: A Scoping Review.AIDS Behav. 2024 Oct;28(10):3381-3403. doi: 10.1007/s10461-024-04436-6. Epub 2024 Jul 11. AIDS Behav. 2024. PMID: 38992228
-
Evaluation of a combination adherence strategy to support HIV antiretroviral therapy for pregnancy and breastfeeding in Malawi: A pilot randomized clinical trial.PLoS One. 2025 Apr 28;20(4):e0319735. doi: 10.1371/journal.pone.0319735. eCollection 2025. PLoS One. 2025. PMID: 40293995 Free PMC article. Clinical Trial.
-
Supply-side readiness to deliver HIV testing and treatment services in Indonesia: Going the last mile to eliminate mother-to-child transmission of HIV.PLOS Glob Public Health. 2022 Aug 3;2(8):e0000845. doi: 10.1371/journal.pgph.0000845. eCollection 2022. PLOS Glob Public Health. 2022. PMID: 36962570 Free PMC article.
References
-
- Aliyu MH, Blevins M, Audet CM, Kalish M, Gebi UI, Onwujekwe O, et al. Integrated prevention of mother‐to‐child HIV transmission services, antiretroviral therapy initiation, and maternal and infant retention in care in rural north‐central Nigeria: a cluster‐randomised controlled trial. Lancet HIV. 2016;3:e202–211. - PMC - PubMed
-
- World Health Organization . Programmatic update: use of antiretroviral drugs for treating pregnant women and preventing HIV infection in infants: executive summary [cited 2019 Oct 20]. Available from: https://apps.who.int/iris/handle/10665/70892
-
- Barker PM, Mphatswe W, Rollins N. Antiretroviral drugs in the cupboard are not enough: the impact of health systems’ performance on mother‐to‐child transmission of HIV. J Acquir Immune Defic Syndr. 2011;56:e45–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
