

Cost-effectiveness of Recurrent Dupuytren Contracture Treatment
- PMID: 33030553
- PMCID: PMC7545302
- DOI: 10.1001/jamanetworkopen.2020.19861
Cost-effectiveness of Recurrent Dupuytren Contracture Treatment
Abstract
Importance: Owing to its tendency to recur, Dupuytren contracture often requires multiple treatments, which places additional economic burden on health care. The likelihood of contracture recurrence varies not only with treatment but also with disease characteristics, such as contracture severity and location, but prior cost-effectiveness analyses of Dupuytren contracture treatments have not considered these patient-specific disease characteristics.
Objective: To identify the most cost-effective treatment regimen for patients with recurrent Dupuytren contracture.
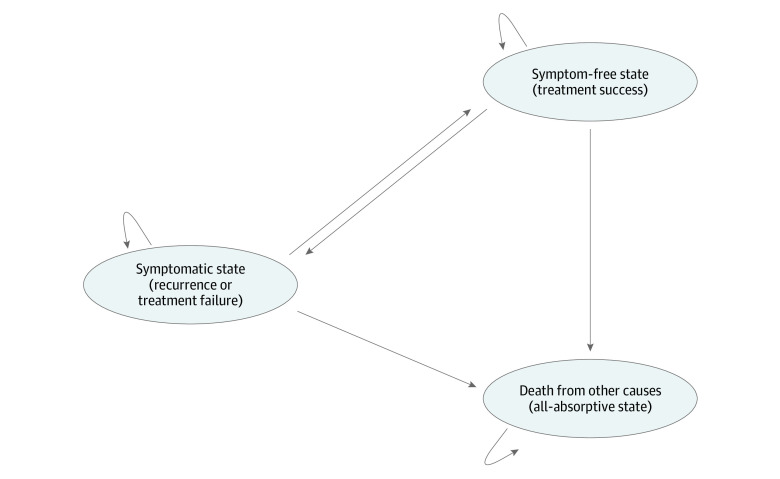
Design, setting, and participants: This economic evaluation was conducted with state-transition microsimulation modeling using data from published studies and Medicare. A simulated cohort of 10 000 individuals with Dupuytren contracture was created. Patients could transition yearly between the following health states: symptom-free, symptomatic, and death. Available treatments were collagenase clostridium histolyticum injection, percutaneous needle aponeurotomy (PNA), and limited fasciectomy (LF); individuals randomly chose any treatment when symptomatic. Patients were limited to 3 rounds of treatment for a contracture affecting 1 joint, totaling 27 unique combinations. If the contracture recurred after 3 treatments, patients lived with the disease for the remainder of life.
Exposures: PNA, collagenase clostridium histolyticum injection, or LF.
Main outcomes and measures: Quality-adjusted life-years (QALYs), total costs (in US dollars), and incremental cost-effectiveness ratios (ICERs). A willingness-to-pay threshold of $100 000 per quality-adjusted life-year was used to assess cost-effectiveness.
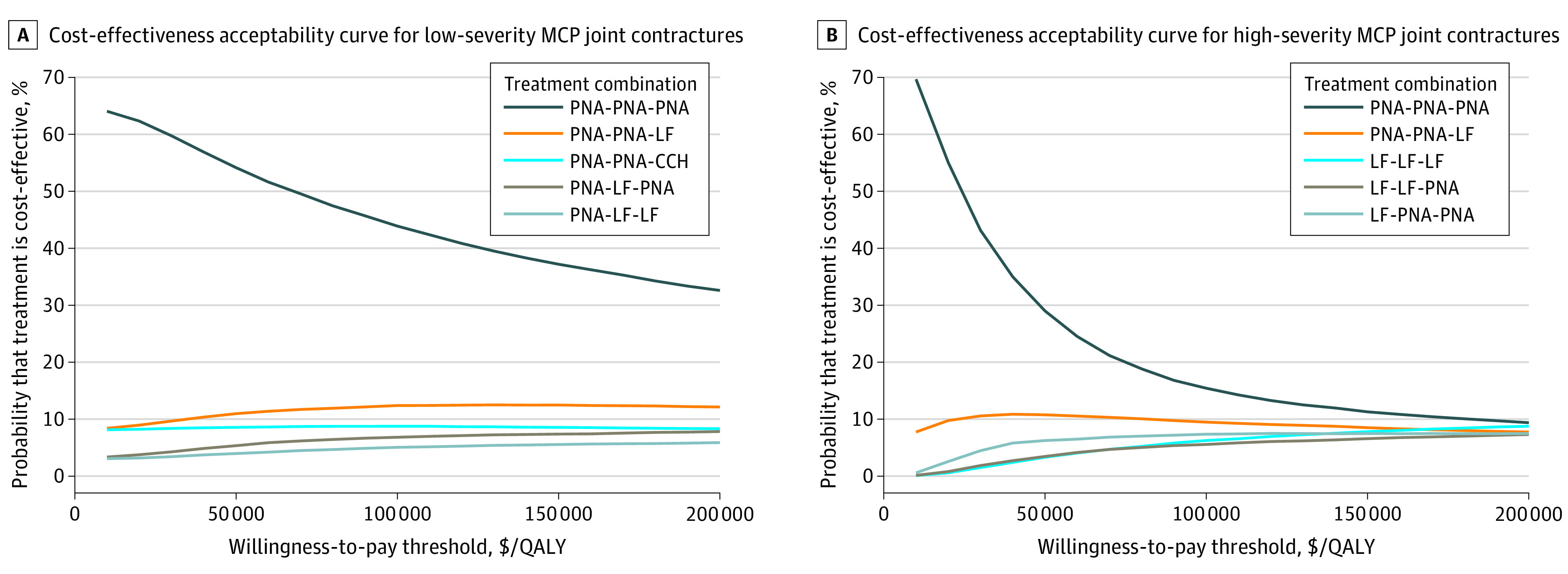
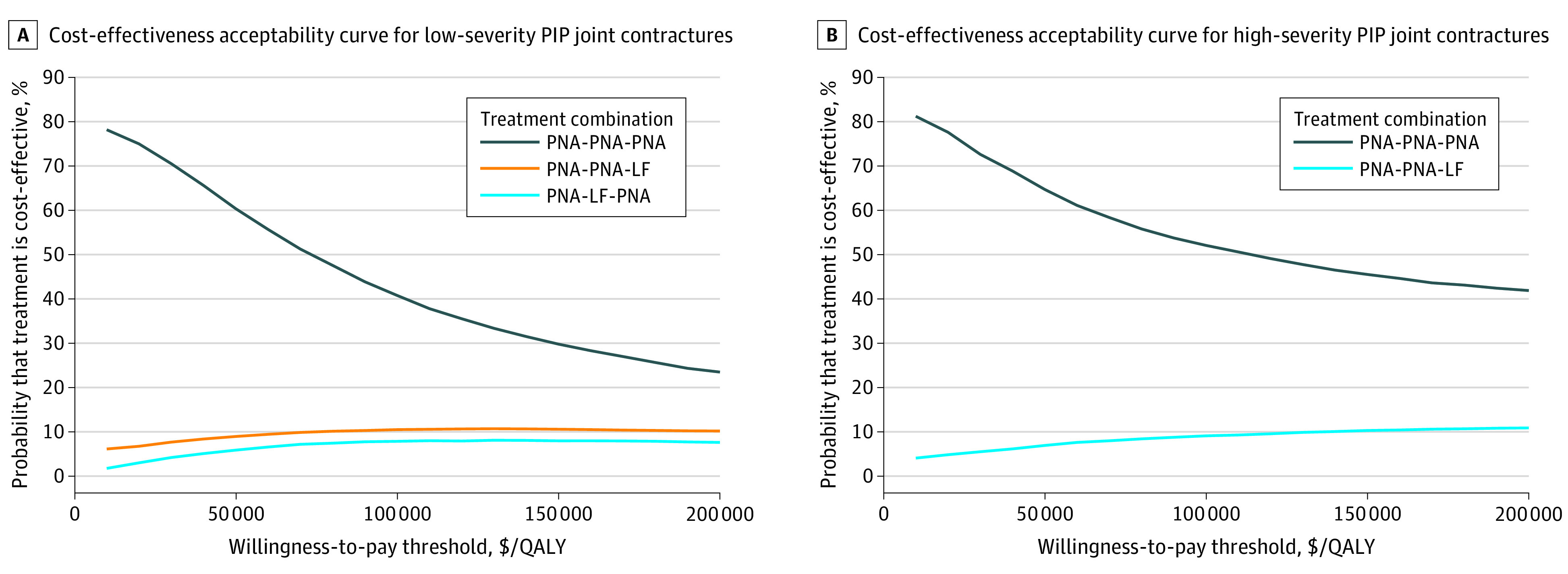
Results: For the base case scenario of a patient aged 60 years with recurrent, low-severity metacarpophalangeal (MCP) joint contracture, repeated PNA treatment was the only cost-effective treatment (2 PNA treatments followed by LF vs 3 PNA treatments, ICER [Monte Carlo SE]: $212 647/QALY [$36 000/QALY]). For recurrent high-severity MCP joint contractures, treatment regimens composed of PNA and LF were cost-effective (ICER [Monte Carlo SE], $93 932/QALY [$16 500/QALY]). LF was cost-effective for high-severity MCP joint contracture (ICER [Monte Carlo SE], $98 624/QALY [$26 233/QALY]). For recurrent proximal interphalangeal (PIP) joint contractures, PNA was the only cost-effective treatment, regardless of severity (eg, 2 PNA treatments followed by LF vs 3 PNA treatments for low-severity PIP joint contracture, ICER [Monte Carlo SE]: $263 726/QALY [$29 000/QALY]). Any combination with collagenase clostridium histolyticum injection compared with 3 PNA treatments had an ICER greater than $100 000 per QALY. Probabilistic sensitivity analysis estimated a 44%, 15%, 41%, and 52% chance of a regimen consisting of only PNA being cost-effective in low-severity MCP, high-severity MCP, low-severity PIP, and high-severity PIP joint contractures, respectively.
Conclusions and relevance: The results of this study suggest that LF is a cost-effective intervention for recurrent high-severity MCP joint contractures. For recurrent low-severity MCP joint contractures and PIP joint contractures of all severity levels, PNA was the only cost-effective intervention. Collagenase clostridium histolyticum injections were not a cost-effective intervention for recurrent Dupuytren contracture and should not be preferred over PNA or LF.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
