

Tumor and germline next generation sequencing in high grade serous cancer: experience from a large population-based testing program
- PMID: 33030818
- PMCID: PMC7782089
- DOI: 10.1002/1878-0261.12817
Tumor and germline next generation sequencing in high grade serous cancer: experience from a large population-based testing program
Erratum in
-
Corrigendum to: Tumor and germline next generation sequencing in high grade serous cancer: experience from a large population-based testing program.Mol Oncol. 2021 Jul;15(7):1970. doi: 10.1002/1878-0261.13018. Epub 2021 May 31. Mol Oncol. 2021. PMID: 34060208 Free PMC article. No abstract available.
Abstract
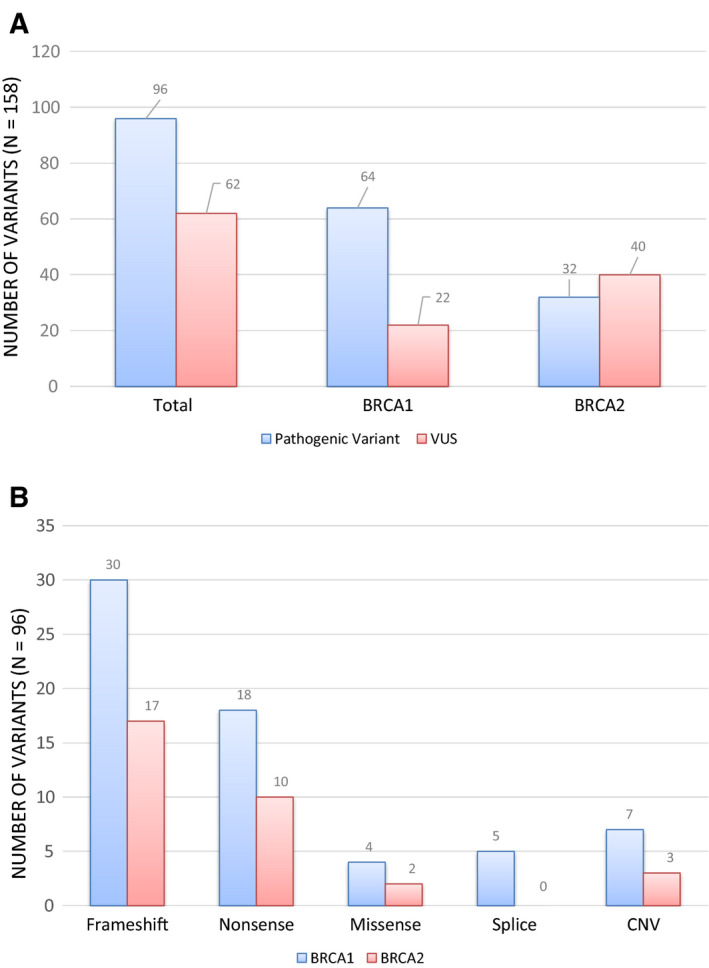
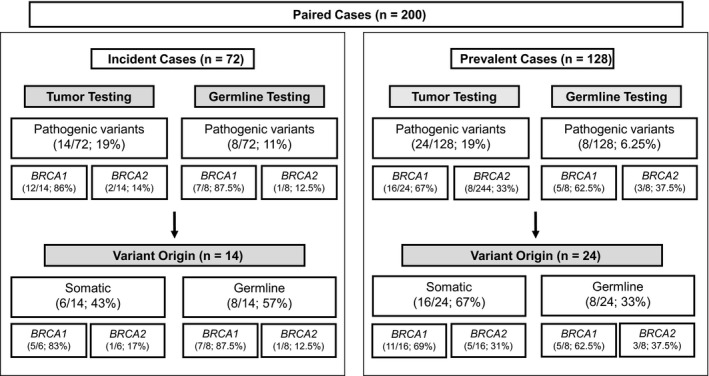
The aim of this study was to determine the prevalence of somatic and germline pathogenic variants (PVs) in high-grade serous cancer (HGSC) and to demonstrate the technical feasibility and effectiveness of a large-scale, population-based tumor testing program. It involved a retrospective review of genetic test results in 600 consecutive HGSC tumor samples and a subsequent comparison of germline and tumor results in a subset of 200 individuals. Tumor testing was successful in 95% of samples (570/600) with at least one BRCA1/2 PV identified in 16% (93/570) of cases. Among the 200 paired cases, BRCA1/2 PVs were detected in 38 tumors (19%); 58% were somatic (22/38); and 42% were germline (16/38). There was 100% concordance between germline and tumor test results. This is the largest series of BRCA1/2 testing in HGSC (tumor-only and paired cohorts), reported to date, and our data show that an effectively designed and validated population-based tumor testing program can be used to determine both treatment eligibility and hereditary cancer risk.
Keywords: BRCA1/BRCA2; germline variant; high-grade serous cancer; next-generation sequencing; somatic variant; tumor testing.
© 2020 The Authors. Molecular Oncology published by John Wiley & Sons Ltd on behalf of Federation of European Biochemical Societies.
Conflict of interest statement
Melanie Care has received speaker honoraria and travel support from AstraZeneca, Inc. Jeanna McCuaig has speaker honoraria and travel support from AstraZeneca, Inc., and speaker honoraria from Pfizer, Inc. Tracy L. Stockley has received funding for test development from AstraZeneca and honoraria for advisory board meetings. All other authors declare no conflicts of interest.
Figures

Similar articles
-
The detection of germline and somatic BRCA1/2 genetic variants through parallel testing of patients with high-grade serous ovarian cancer: a national retrospective audit.BJOG. 2022 Feb;129(3):433-442. doi: 10.1111/1471-0528.16975. Epub 2021 Nov 8. BJOG. 2022. PMID: 34657373 Free PMC article.
-
Mutation landscape of germline and somatic BRCA1/2 in patients with high-grade serous ovarian cancer.BMC Cancer. 2020 Mar 12;20(1):204. doi: 10.1186/s12885-020-6693-y. BMC Cancer. 2020. PMID: 32164585 Free PMC article.
-
Invasion Patterns of Metastatic Extrauterine High-grade Serous Carcinoma With BRCA Germline Mutation and Correlation With Clinical Outcomes.Am J Surg Pathol. 2016 Mar;40(3):404-9. doi: 10.1097/PAS.0000000000000556. Am J Surg Pathol. 2016. PMID: 26574845 Free PMC article.
-
[Detecting Large Germline Rearrangements of BRCA1 by Next Generation Tumor Sequencing].Mol Biol (Mosk). 2020 May-Jun;54(4):688-698. doi: 10.31857/S0026898420040114. Mol Biol (Mosk). 2020. PMID: 32840490 Review. Russian.
-
[Oncopathological aspects of BRCA1 and BRCA2 genes inactivation in tumors of ovary, fallopian tube and pelvic peritoneum].Cesk Patol. 2016 Fall;52(4):199-204. Cesk Patol. 2016. PMID: 27869446 Review. Czech.
Cited by
-
VHL mosaicism: the added value of multi-tissue analysis.NPJ Genom Med. 2022 Mar 18;7(1):21. doi: 10.1038/s41525-022-00291-3. NPJ Genom Med. 2022. PMID: 35304467 Free PMC article.
-
A commentary on the discrepancy between blood and tumour BRCA testing: An open question.BJOG. 2022 Aug;129(9):1422-1426. doi: 10.1111/1471-0528.17158. Epub 2022 Apr 5. BJOG. 2022. PMID: 35319826 Free PMC article. No abstract available.
-
Homologous Recombination Deficiency (HRD) Scoring, by Means of Two Different Shallow Whole-Genome Sequencing Pipelines (sWGS), in Ovarian Cancer Patients: A Comparison with Myriad MyChoice Assay.Int J Mol Sci. 2023 Dec 4;24(23):17095. doi: 10.3390/ijms242317095. Int J Mol Sci. 2023. PMID: 38069422 Free PMC article.
-
Practice guidelines for BRCA1/2 tumour testing in ovarian cancer.J Med Genet. 2022 Aug;59(8):727-736. doi: 10.1136/jmedgenet-2021-108238. Epub 2022 Apr 7. J Med Genet. 2022. PMID: 35393334 Free PMC article. Review.
-
Implementation of preventive and predictive BRCA testing in patients with breast, ovarian, pancreatic, and prostate cancer: a position paper of Italian Scientific Societies.ESMO Open. 2022 Jun;7(3):100459. doi: 10.1016/j.esmoop.2022.100459. Epub 2022 May 19. ESMO Open. 2022. PMID: 35597177 Free PMC article. Review.
References
-
- Ledermann JA, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, Scott CL, Meier W, Shapira‐Frommer R, Safra T et al (2014) Olaparib maintenance therapy in patients with platinum sensitive relapsed serous ovarian cancer: a preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol 15, 852–861. - PubMed
-
- Ledermann JA, Harter P, Gourley C, Friedlander M, Vergote I, Rustin G, Scott C, Meier W, Shapira‐Frommer R, Safra T et al (2016) Overall survival in patients with platinum‐sensitive recurrent serous ovarian cancer receiving olaparib maintenance monotherapy: an updated analysis from a randomised, placebo‐controlled, double‐blind, phase 2 trial. Lancet Oncol 17, 1579–1589. - PubMed
-
- Swisher EM, Lin KK, Oza AM, Scott CL, Giordano H, Sun J, Konecny GE, Coleman RL, Tinker AV, O'Malley DM et al (2017) Rucaparib in relapsed, platinum‐sensitive high‐grade ovarian carcinoma (ARIEL2 Part 1): an international, multicentre, open‐label, phase 2 trial. Lancet Oncol 18, 75–87. - PubMed
-
- Pujade‐Lauraine E, Ledermann JA, Selle F, Gebski V, Penson RT, Oza AM, Korach J, Huzarski T, Poveda A, Pignata S et al (2017) Olaparib tablets as maintenance therapy in patients with platinum‐sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT‐Ov21): a double‐blind, randomised, placebo‐controlled, phase 3 trial. Lancet Oncol 18, 1274–1284. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
