

FOXP3 mRNA Profile Prognostic of Acute T Cell-mediated Rejection and Human Kidney Allograft Survival
- PMID: 33031221
- PMCID: PMC8024419
- DOI: 10.1097/TP.0000000000003478
FOXP3 mRNA Profile Prognostic of Acute T Cell-mediated Rejection and Human Kidney Allograft Survival
Abstract
Background: T cell-mediated rejection (TCMR) is the most frequent type of acute rejection and is associated with kidney allograft failure. Almost 40% of TCMR episodes are nonresponsive to therapy, and molecular mechanisms for the nonresponsiveness are unknown. Our single-center study identified that urinary cell FOXP3 mRNA abundance predicts TCMR reversibility and allograft survival.
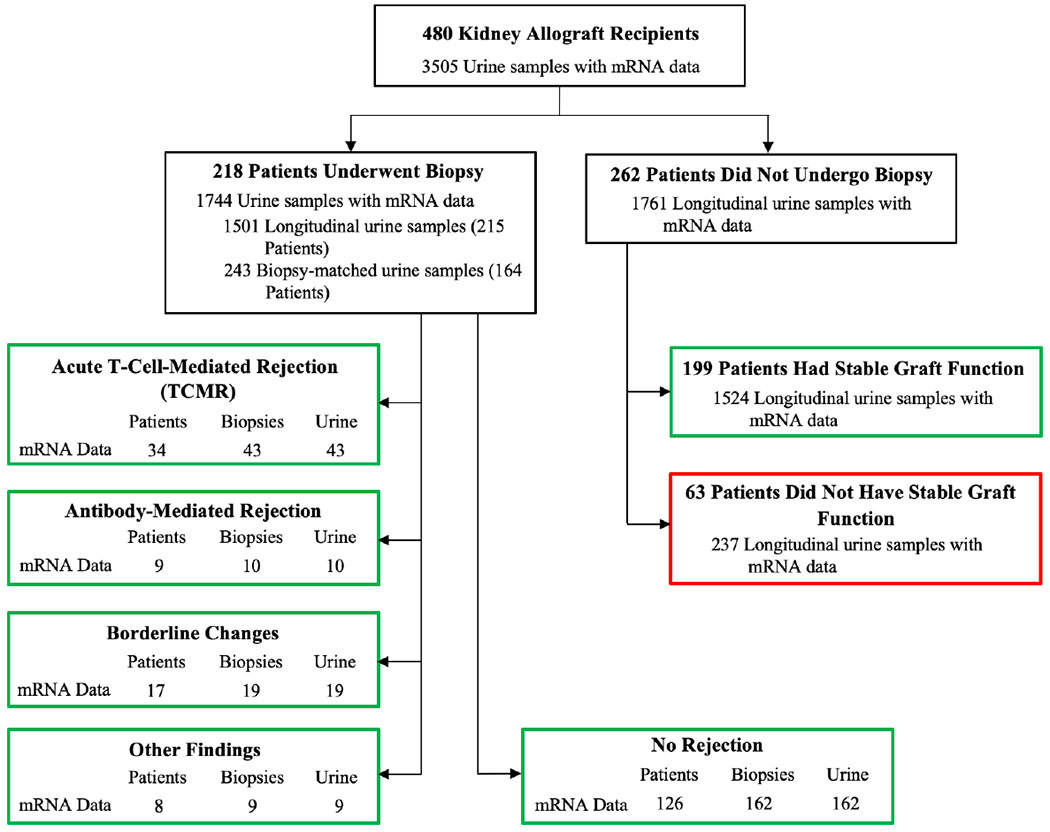
Methods: We developed PCR assays and measured absolute copy numbers of transcripts for FOXP3, CD25, CD3E, perforin, and 18S rRNA in 3559 urines from 480 kidney allograft recipients prospectively enrolled in the multicenter Clinical Trials in Organ Transplantation-04. In this replication study, we investigated the association between mRNA profile and TCMR diagnosis, TCMR reversibility, and allograft survival.
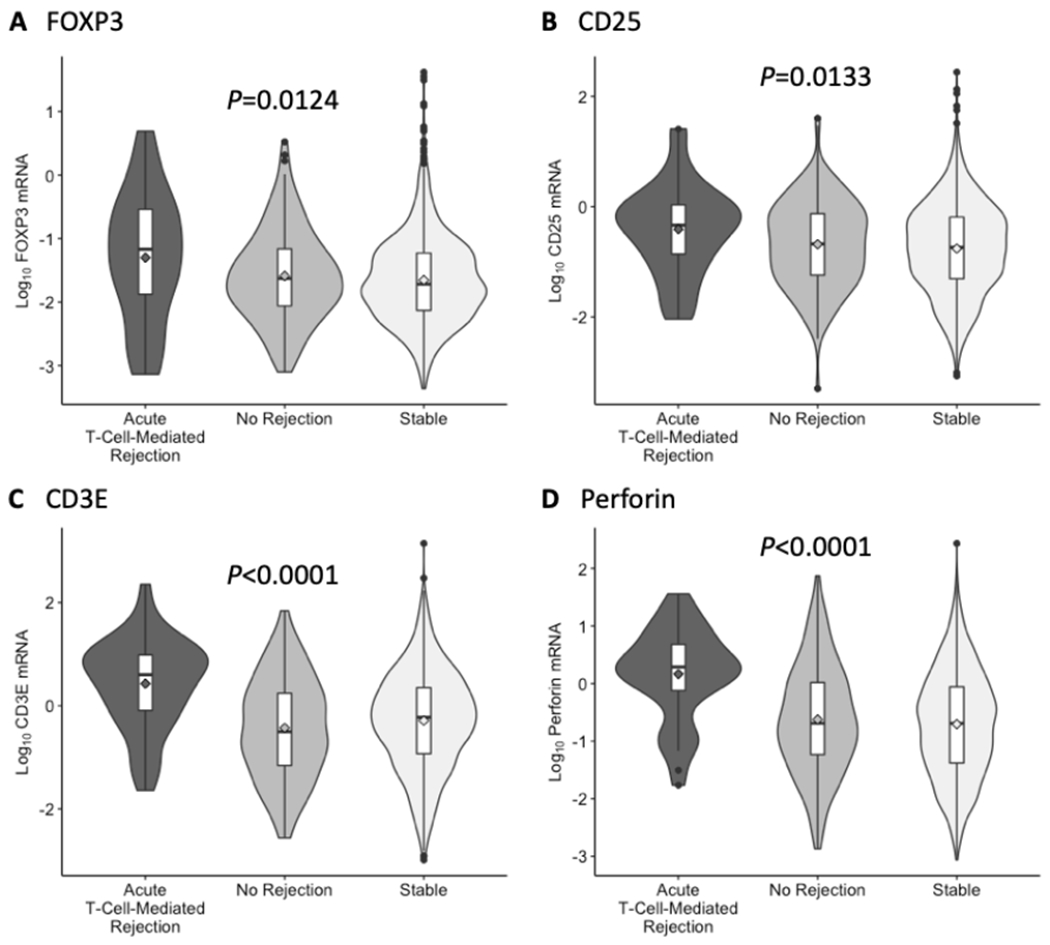
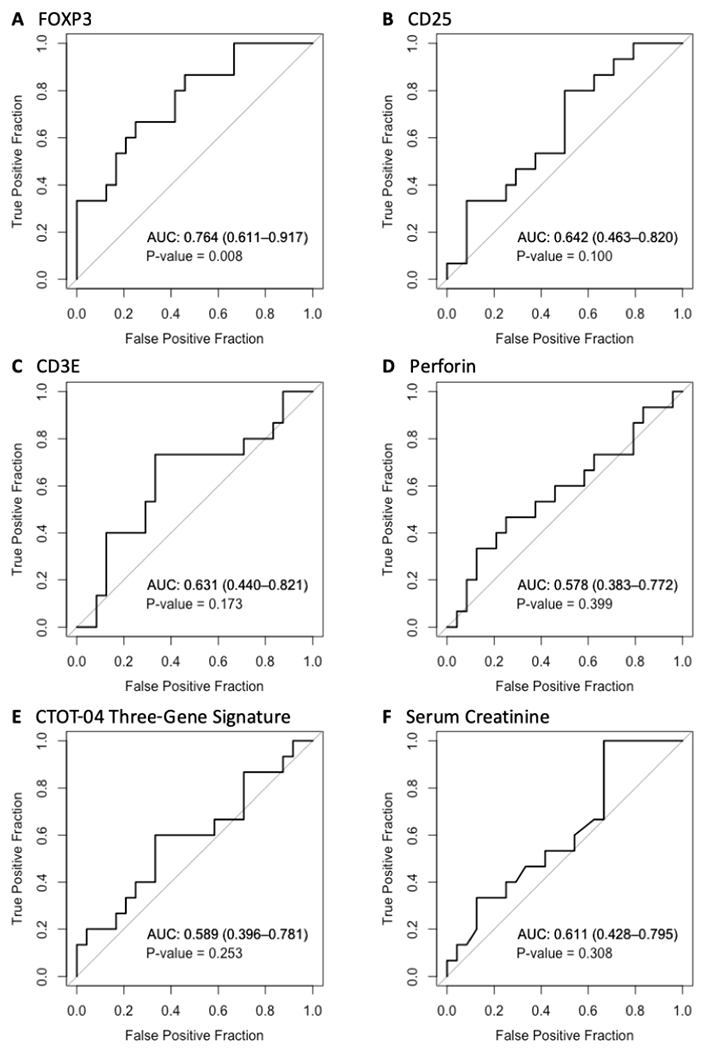
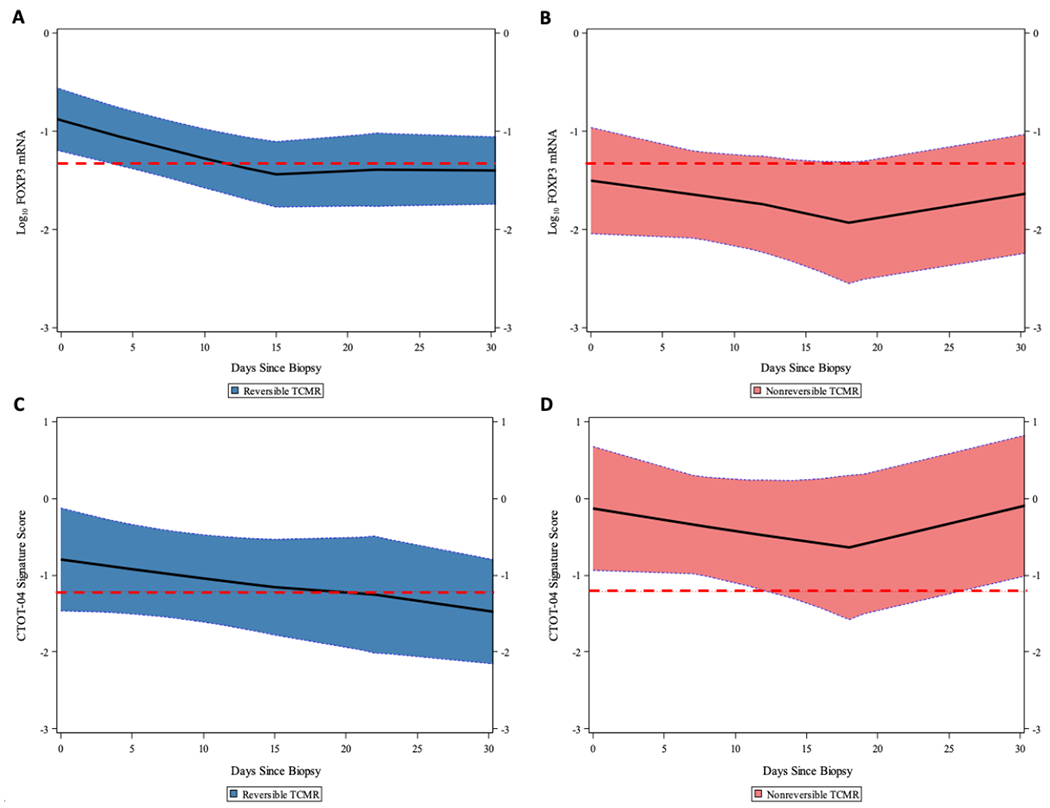
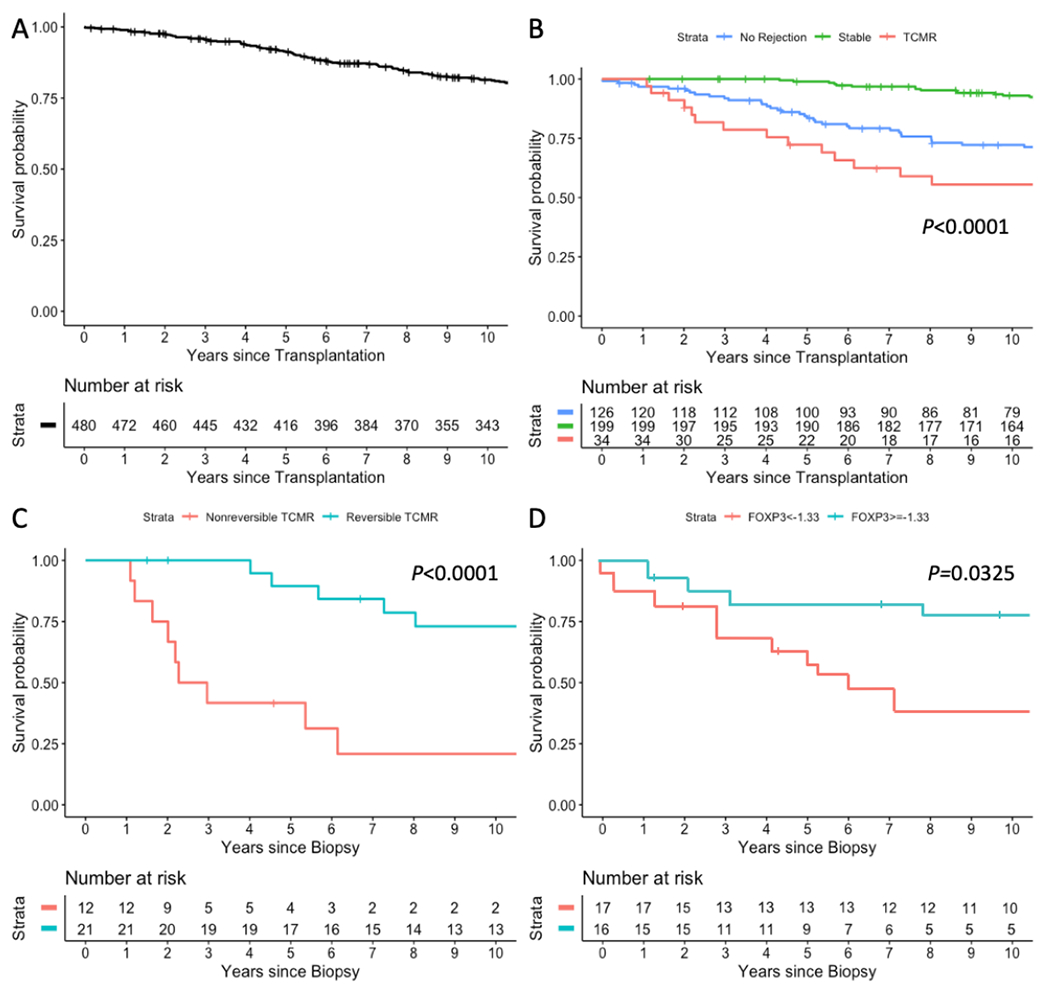
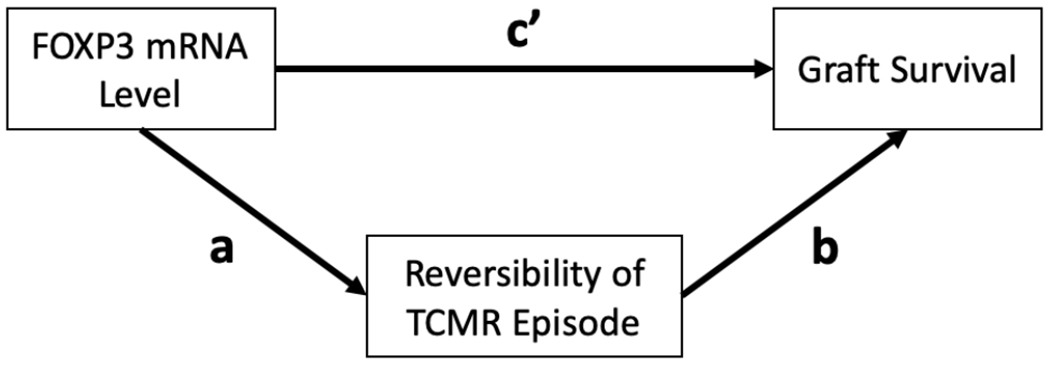
Results: 18S rRNA normalized levels of mRNA for FOXP3 (P = 0.01, Kruskal-Wallis test), CD25 (P = 0.01), CD3E (P < 0.0001), and perforin (P < 0.0001) were diagnostic of TCMR, but only FOXP3 mRNA level predicted TCMR reversibility (ROC AUC = 0.764; 95% confidence interval, 0.611-0.917; P = 0.008). Multivariable logistic regression analyses showed that urinary cell FOXP3 mRNA level predicted reversal, independent of clinical variables. A composite model of clinical variables and FOXP3 mRNA (AUC = 0.889; 95% CI, 0.781-0.997; P < 0.001) outperformed FOXP3 mRNA or clinical variables in predicting TCMR reversibility (P = 0.01, likelihood ratio test). Multivariable Cox proportional hazards regression analyses showed that FOXP3 mRNA level predicts kidney allograft survival (P = 0.047) but not after controlling for TCMR reversal (P = 0.477).
Conclusions: Urinary cell level of FOXP3 mRNA is diagnostic of TCMR, predicts TCMR reversibility, and is prognostic of kidney allograft survival via a mechanism involving TCMR reversal.
Copyright © 2020 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
M.S. has a Consultancy Agreement with CareDx, Inc., Brisbane, CA, and with Sparks Therapeutics, Philadelphia, PA. The other authors of this manuscript declare no conflicts of interest.
Figures
Comment in
-
Outfoxing Rejection: Urinary FOXP3 mRNA, TCMR, and the Fate of Allografts.Transplantation. 2021 Aug 1;105(8):1662-1663. doi: 10.1097/TP.0000000000003479. Transplantation. 2021. PMID: 33031219 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
