

What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors
- PMID: 33031427
- PMCID: PMC7544065
- DOI: 10.1371/journal.pone.0240205
What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors
Abstract
Introduction: Current SARS-CoV-2 containment measures rely on controlling viral transmission. Effective prioritization can be determined by understanding SARS-CoV-2 transmission dynamics. We conducted a systematic review and meta-analyses of the secondary attack rate (SAR) in household and healthcare settings. We also examined whether household transmission differed by symptom status of index case, adult and children, and relationship to index case.
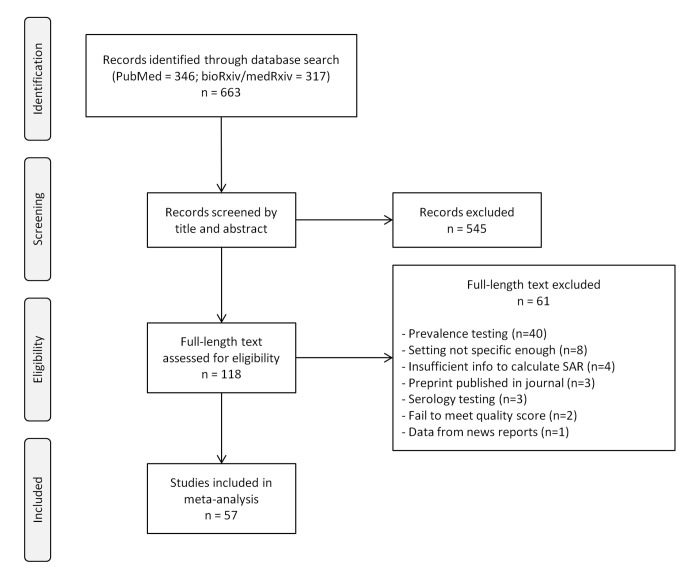
Methods: We searched PubMed, medRxiv, and bioRxiv databases between January 1 and July 25, 2020. High-quality studies presenting original data for calculating point estimates and 95% confidence intervals (CI) were included. Random effects models were constructed to pool SAR in household and healthcare settings. Publication bias was assessed by funnel plots and Egger's meta-regression test.
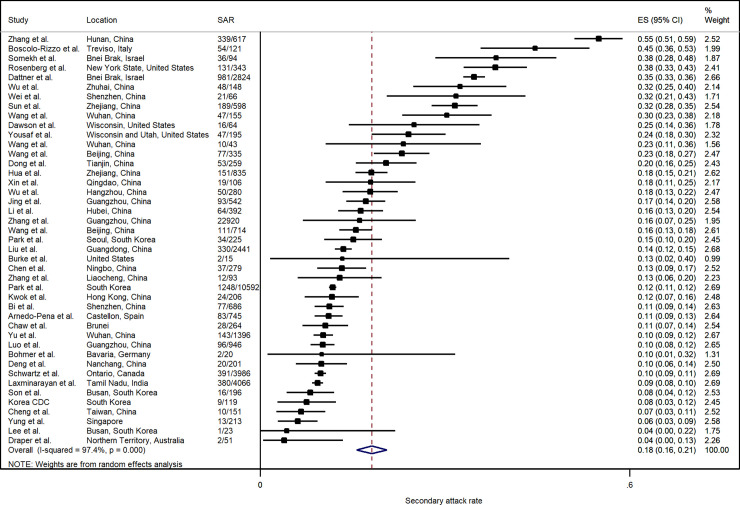
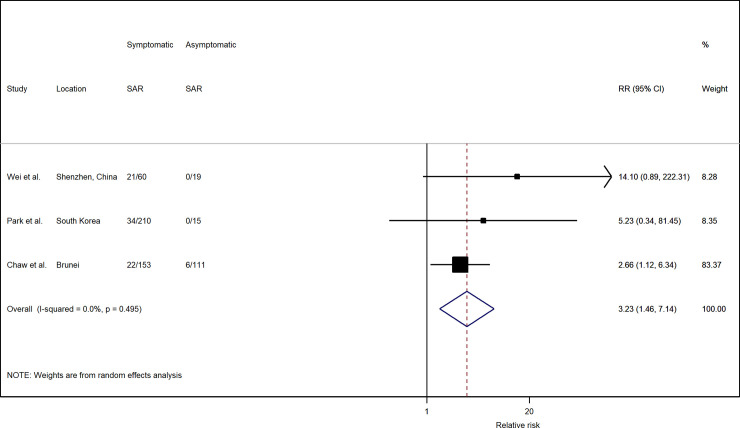
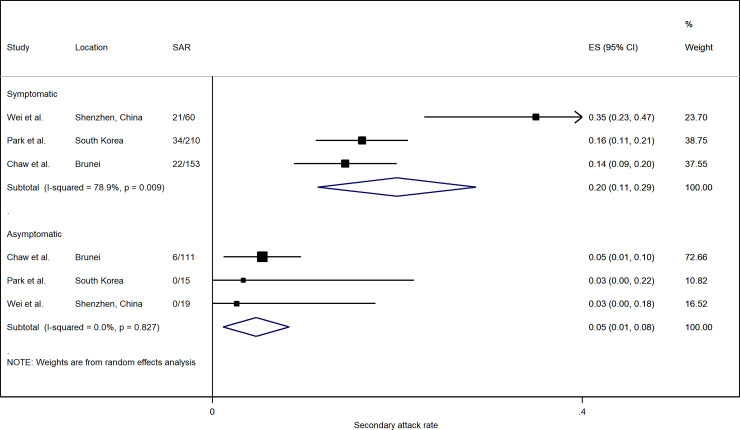
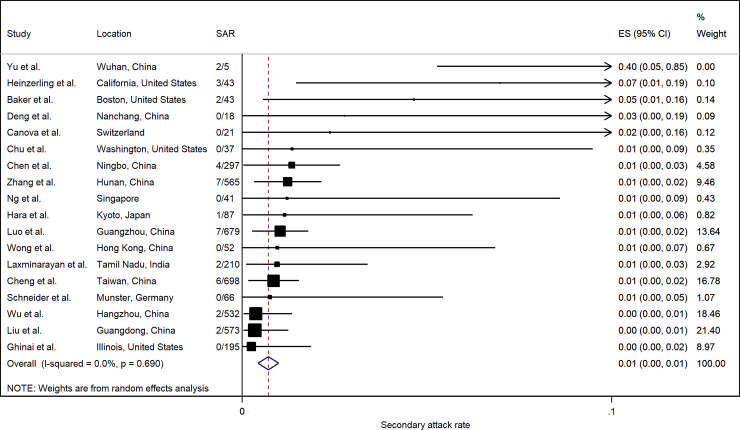
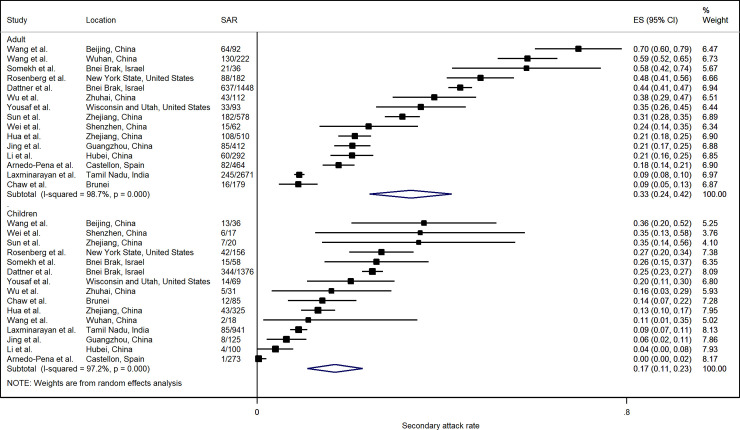
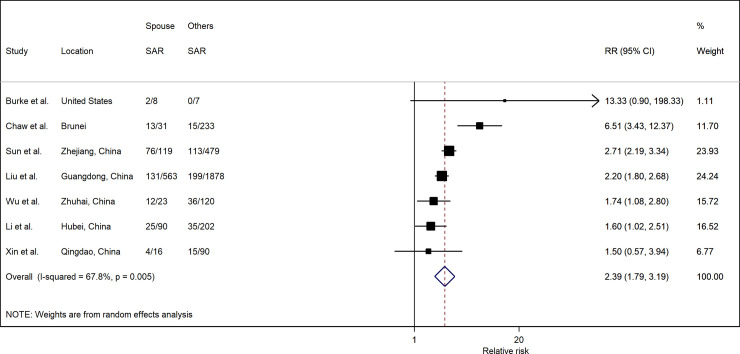
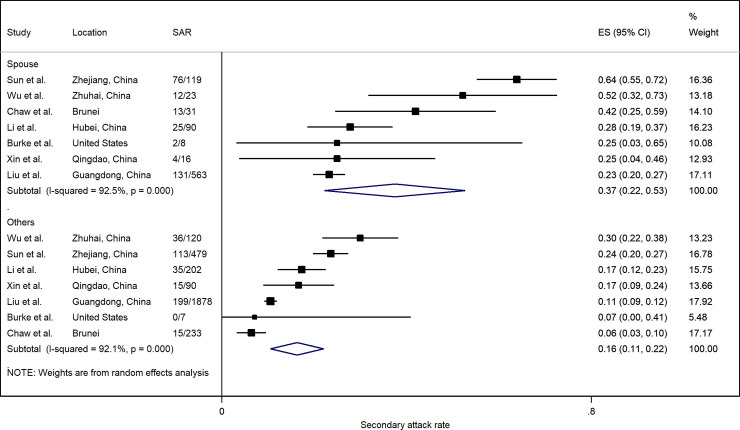
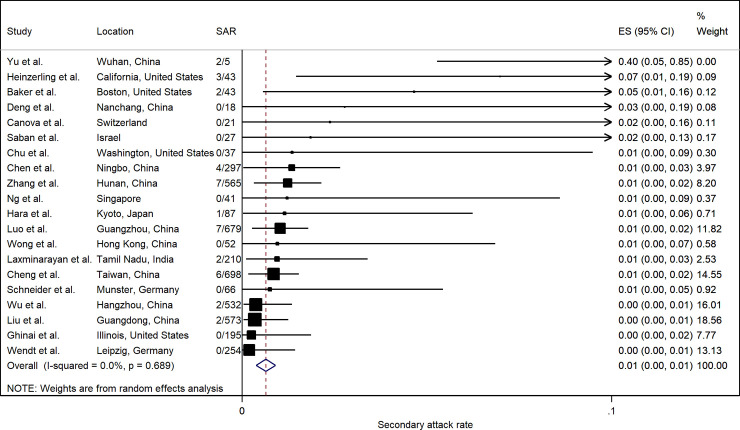
Results: 43 studies met the inclusion criteria for household SAR, 18 for healthcare SAR, and 17 for other settings. The pooled household SAR was 18.1% (95% CI: 15.7%, 20.6%), with significant heterogeneity across studies ranging from 3.9% to 54.9%. SAR of symptomatic index cases was higher than asymptomatic cases (RR: 3.23; 95% CI: 1.46, 7.14). Adults showed higher susceptibility to infection than children (RR: 1.71; 95% CI: 1.35, 2.17). Spouses of index cases were more likely to be infected compared to other household contacts (RR: 2.39; 95% CI: 1.79, 3.19). In healthcare settings, SAR was estimated at 0.7% (95% CI: 0.4%, 1.0%).
Discussion: While aggressive contact tracing strategies may be appropriate early in an outbreak, as it progresses, measures should transition to account for setting-specific transmission risk. Quarantine may need to cover entire communities while tracing shifts to identifying transmission hotspots and vulnerable populations. Where possible, confirmed cases should be isolated away from the household.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lurie N, Saville M, Hatchett R, Halton J. Developing Covid-19 Vaccines at Pandemic Speed. N Engl J Med. 2020. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
