

Association of SGLT2 Inhibitors With Cardiovascular and Kidney Outcomes in Patients With Type 2 Diabetes: A Meta-analysis
- PMID: 33031522
- PMCID: PMC7542529
- DOI: 10.1001/jamacardio.2020.4511
Association of SGLT2 Inhibitors With Cardiovascular and Kidney Outcomes in Patients With Type 2 Diabetes: A Meta-analysis
Abstract
Importance: Sodium-glucose cotransporter 2 (SGLT2) inhibitors favorably affect cardiovascular (CV) and kidney outcomes; however, the consistency of outcomes across the class remains uncertain.
Objective: To perform meta-analyses that assess the CV and kidney outcomes of all 4 available SGLT2 inhibitors in patients with type 2 diabetes.
Data sources: A systematic literature search was conducted in PubMed from January 1, 2015, to January 31, 2020.
Study selection: One hundred forty-five records were initially identified; 137 were excluded because of study design or topic of interest. As a result, a total of 6 randomized, placebo-controlled CV and kidney outcomes trials of SGLT2 inhibitors in patients with type 2 diabetes were identified, with contributory data from 9 publications. All analyses were conducted on the total patient population of these trials.
Data extraction and synthesis: Standardized data search and abstraction were performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Statement. Data were analyzed using a fixed-effect model.
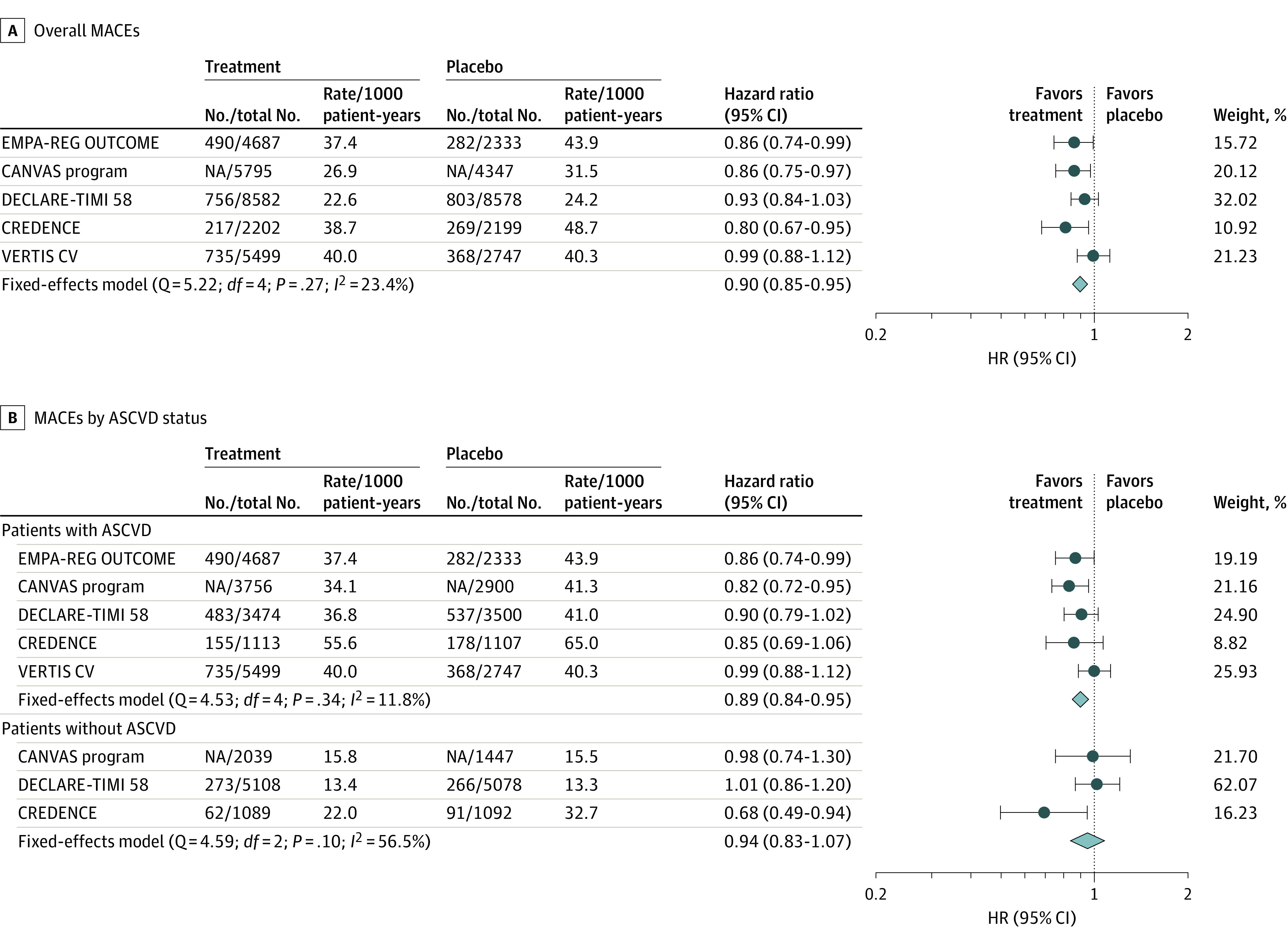
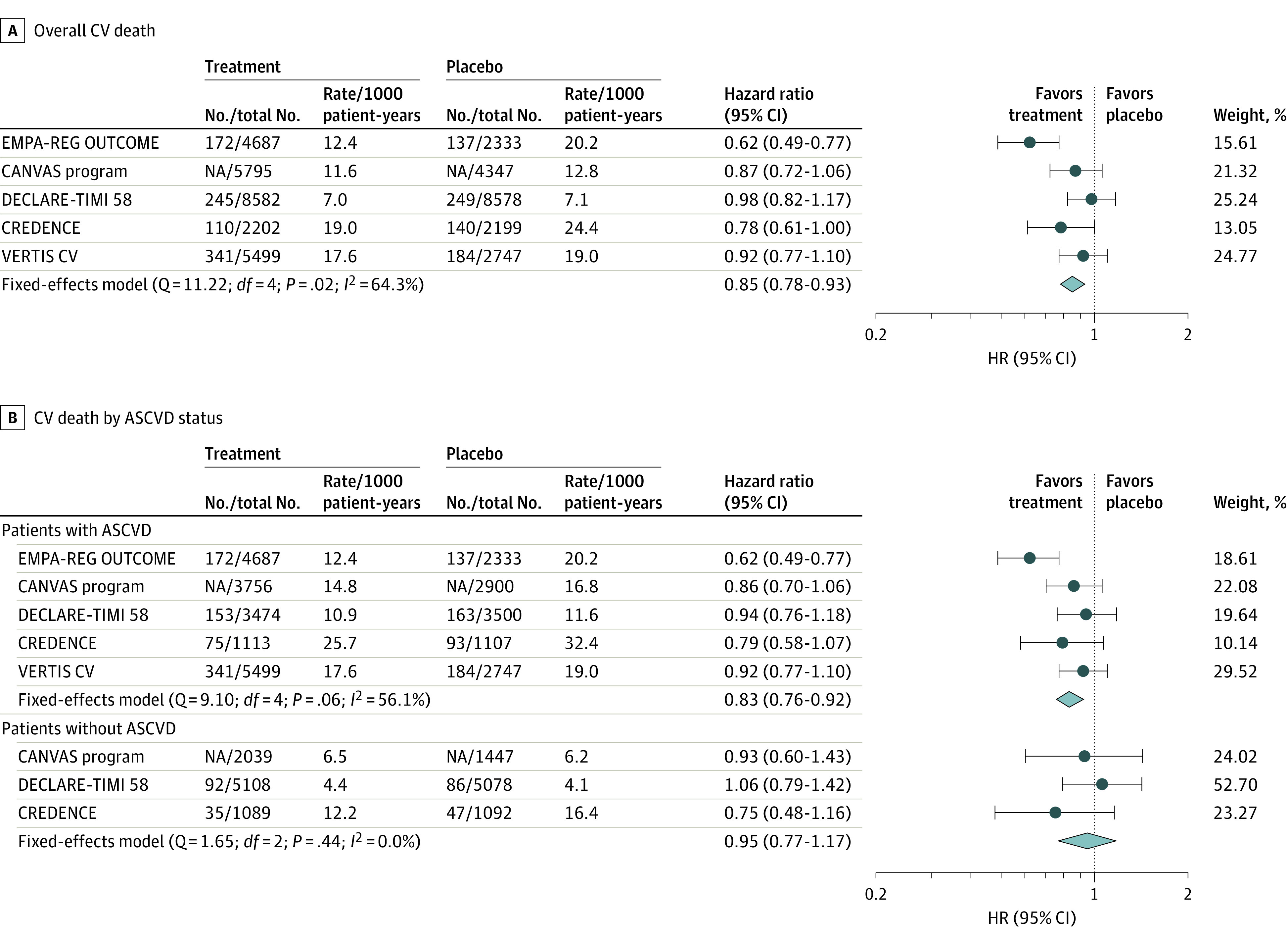
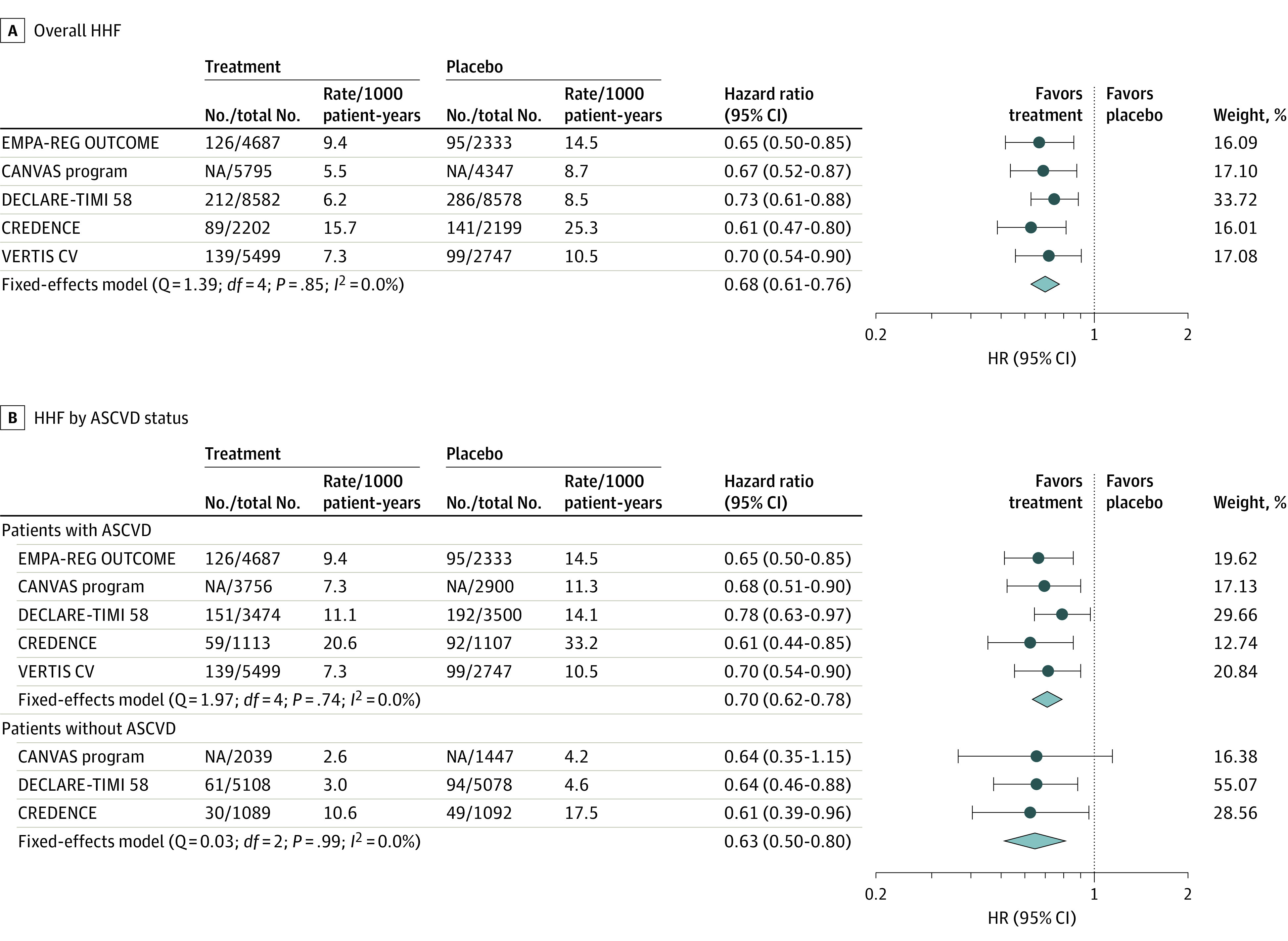
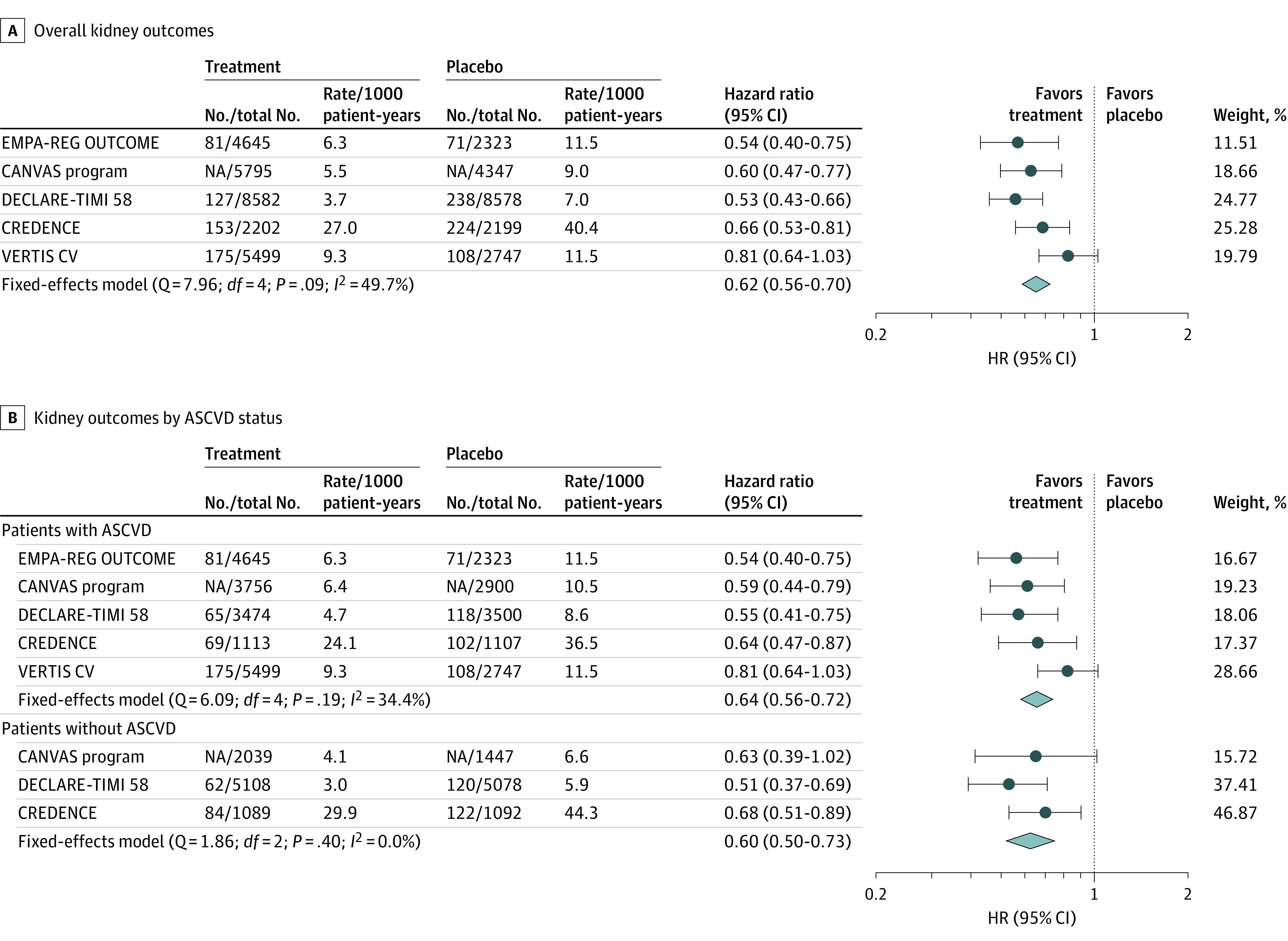
Main outcomes and measures: Outcomes included time to the first event of (1) the composite of major adverse CV events of myocardial infarction, stroke, or CV death, and each component, (2) the composite of hospitalization for heart failure (HHF) or CV death (HHF/CV death) and each component, and (3) kidney composite outcomes. For outcomes in the overall trial populations and in selected subgroups, hazard ratios (HRs) and 95% CIs were pooled and meta-analyzed across trials.
Results: Data from 6 trials comprised 46 969 unique patients with type 2 diabetes, including 31 116 (66.2%) with atherosclerotic CV disease. The mean (SD) age of all trial participants was 63.7 (7.9) years; 30 939 (65.9%) were men, and 36 849 (78.5%) were White. The median number of participants per trial was 8246 (range, 4401-17 160). Overall, SGLT2 inhibitors were associated with a reduced risk of major adverse CV events (HR, 0.90; 95% CI, 0.85-0.95; Q statistic, P = .27), HHF/CV death (HR, 0.78; 95% CI, 0.73-0.84; Q statistic, P = .09), and kidney outcomes (HR, 0.62; 95% CI, 0.56-0.70; Q statistic, P = .09), with no significant heterogeneity of associations with outcome. Associated risk reduction for HHF was consistent across the trials (HR, 0.68; 95% CI, 0.61-0.76; I2 = 0.0%), whereas significant heterogeneity of associations with outcome was observed for CV death (HR, 0.85; 95% CI, 0.78-0.93; Q statistic, P = .02; I2 = 64.3%). The presence or absence of atherosclerotic CV disease did not modify the association with outcomes for major adverse CV events (HR, 0.89; 95% CI, 0.84-0.95 and HR, 0.94; 95% CI, 0.83-1.07, respectively; P = .63 for interaction), with similar absence of associations with outcome modification by prevalent atherosclerotic CV disease for HHF/CV death (P = .62 for interaction), HHF (P = .26 for interaction), or kidney outcomes (P = .73 for interaction).
Conclusions and relevance: In this meta-analysis, SGLT2 inhibitors were associated with a reduced risk of major adverse CV events; in addition, results suggest significant heterogeneity in associations with CV death. The largest benefit across the class was for an associated reduction in risk for HHF and kidney outcomes, with benefits for HHF risk being the most consistent observation across the trials.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
