

Prevalence and Outcome of COVID-19 Infection in Cancer Patients: A National Veterans Affairs Study
- PMID: 33031532
- PMCID: PMC7665587
- DOI: 10.1093/jnci/djaa159
Prevalence and Outcome of COVID-19 Infection in Cancer Patients: A National Veterans Affairs Study
Abstract
Background: Emerging data suggest variability in susceptibility and outcome to coronavirus disease 2019 (COVID-19) infection. Identifying risk factors associated with infection and outcomes in cancer patients is necessary to develop healthcare recommendations.
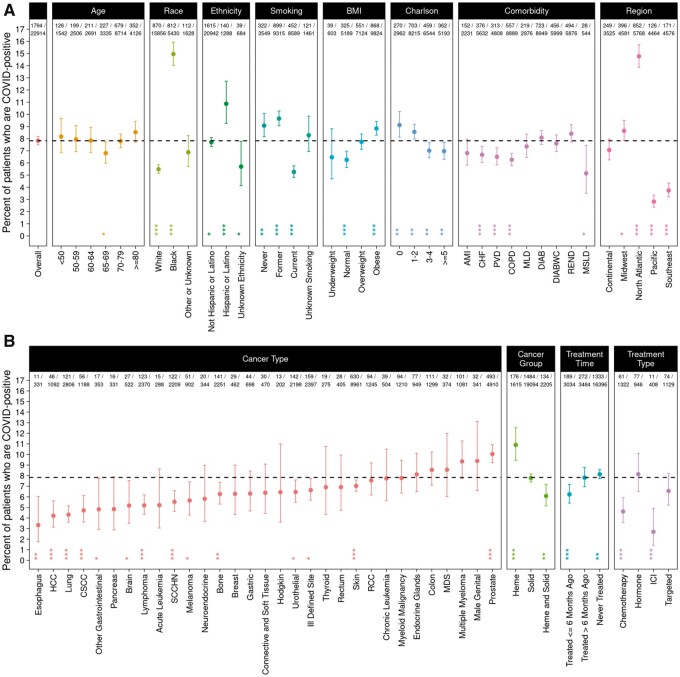
Methods: We analyzed electronic health records of the US Veterans Affairs Healthcare System and assessed the prevalence of COVID-19 infection in cancer patients. We evaluated the proportion of cancer patients tested for COVID-19 who were positive, as well as outcome attributable to COVID-19, and stratified by clinical characteristics including demographics, comorbidities, cancer treatment, and cancer type. All statistical tests are 2-sided.
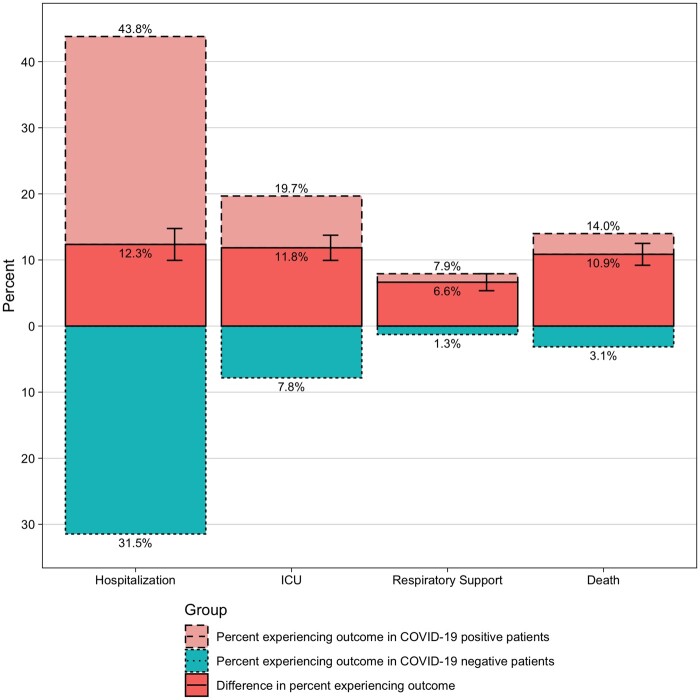
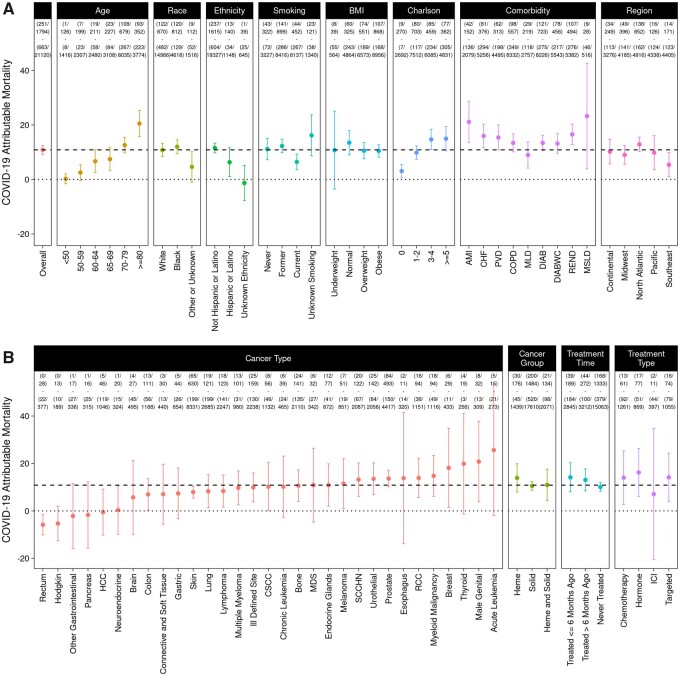
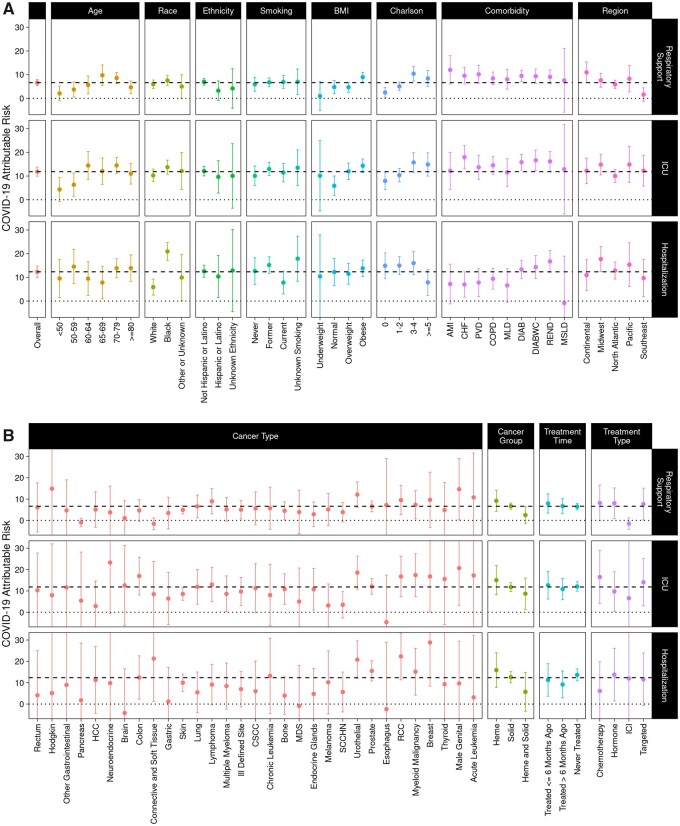
Results: Of 22 914 cancer patients tested for COVID-19, 1794 (7.8%) were positive. The prevalence of COVID-19 was similar across age. Higher prevalence was observed in African American (15.0%) compared with White (5.5%; P < .001) and in patients with hematologic malignancy compared with those with solid tumors (10.9% vs 7.8%; P < .001). Conversely, prevalence was lower in current smokers and patients who recently received cancer therapy (<6 months). The COVID-19-attributable mortality was 10.9%. Higher attributable mortality rates were observed in older patients, those with higher Charlson comorbidity score, and in certain cancer types. Recent (<6 months) or past treatment did not influence attributable mortality. Importantly, African American patients had 3.5-fold higher COVID-19-attributable hospitalization; however, they had similar attributable mortality as White patients.
Conclusion: Preexistence of cancer affects both susceptibility to COVID-19 infection and eventual outcome. The overall COVID-19-attributable mortality in cancer patients is affected by age, comorbidity, and specific cancer types; however, race or recent treatment including immunotherapy do not impact outcome.
Published by Oxford University Press 2020.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
