

Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study
- PMID: 33032450
- PMCID: PMC7688081
- DOI: 10.1161/CIRCULATIONAHA.120.048792
Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study
Abstract
Background: Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is increasingly used to treat cardiogenic shock. However, VA-ECMO might hamper myocardial recovery. The Impella unloads the left ventricle. This study aimed to evaluate whether left ventricular unloading in patients with cardiogenic shock treated with VA-ECMO was associated with lower mortality.
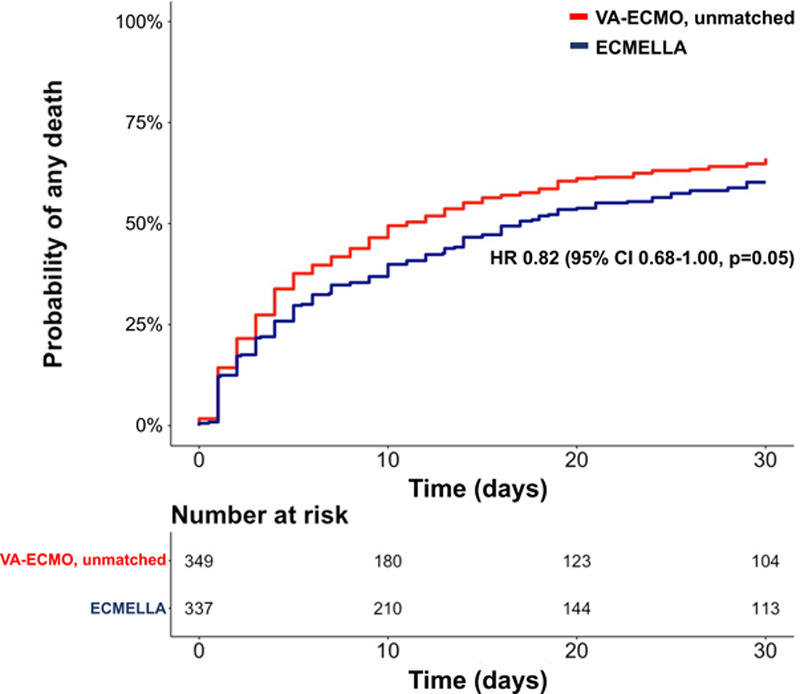
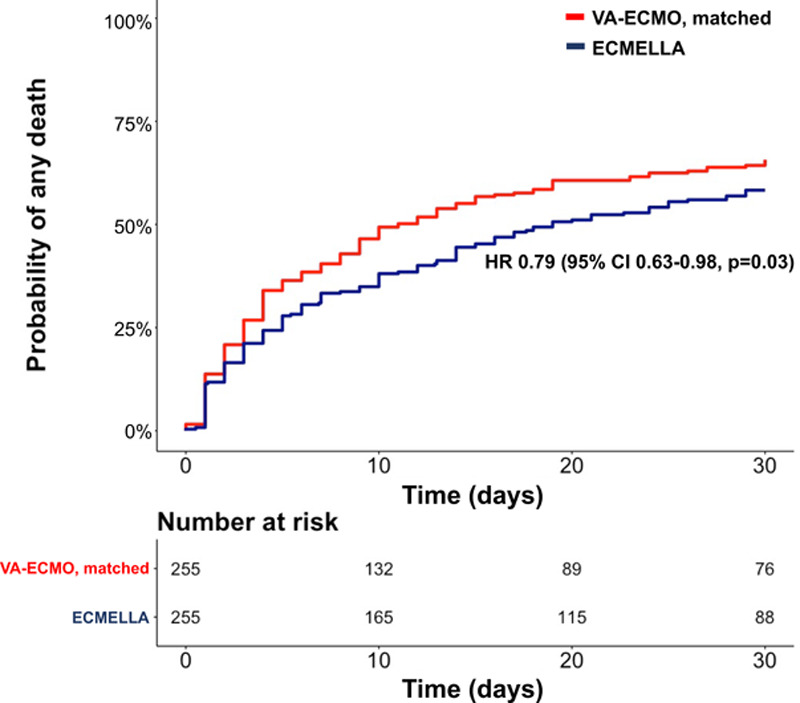
Methods: Data from 686 consecutive patients with cardiogenic shock treated with VA-ECMO with or without left ventricular unloading using an Impella at 16 tertiary care centers in 4 countries were collected. The association between left ventricular unloading and 30-day mortality was assessed by Cox regression models in a 1:1 propensity score-matched cohort.
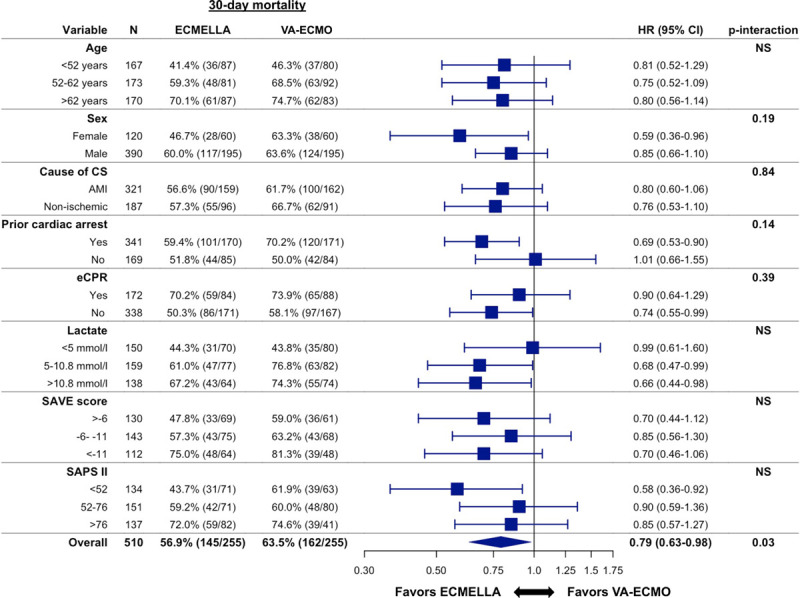
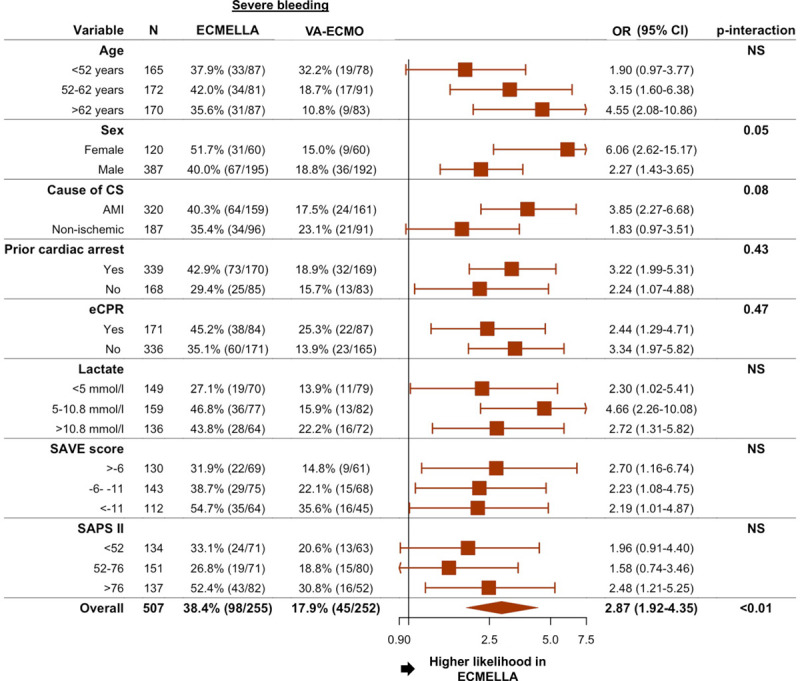
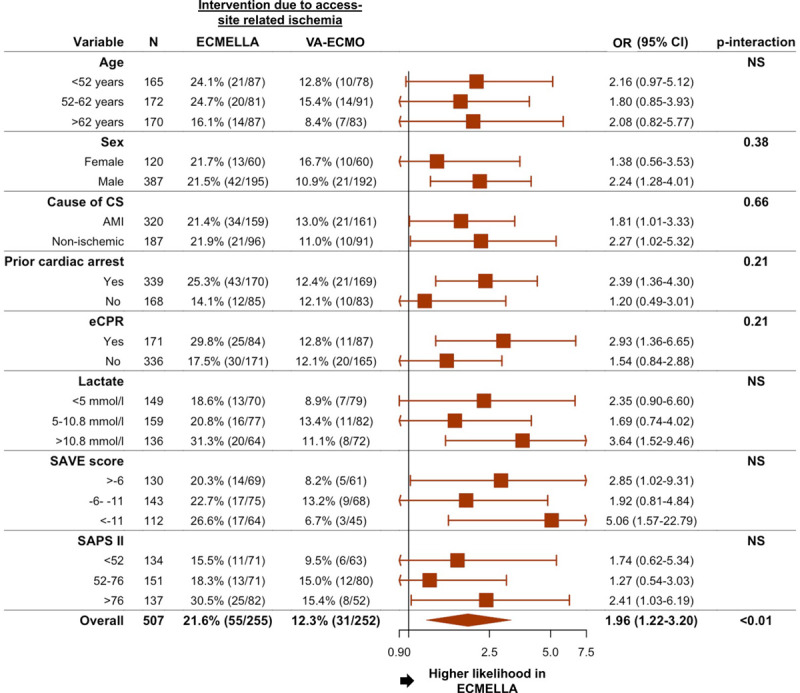
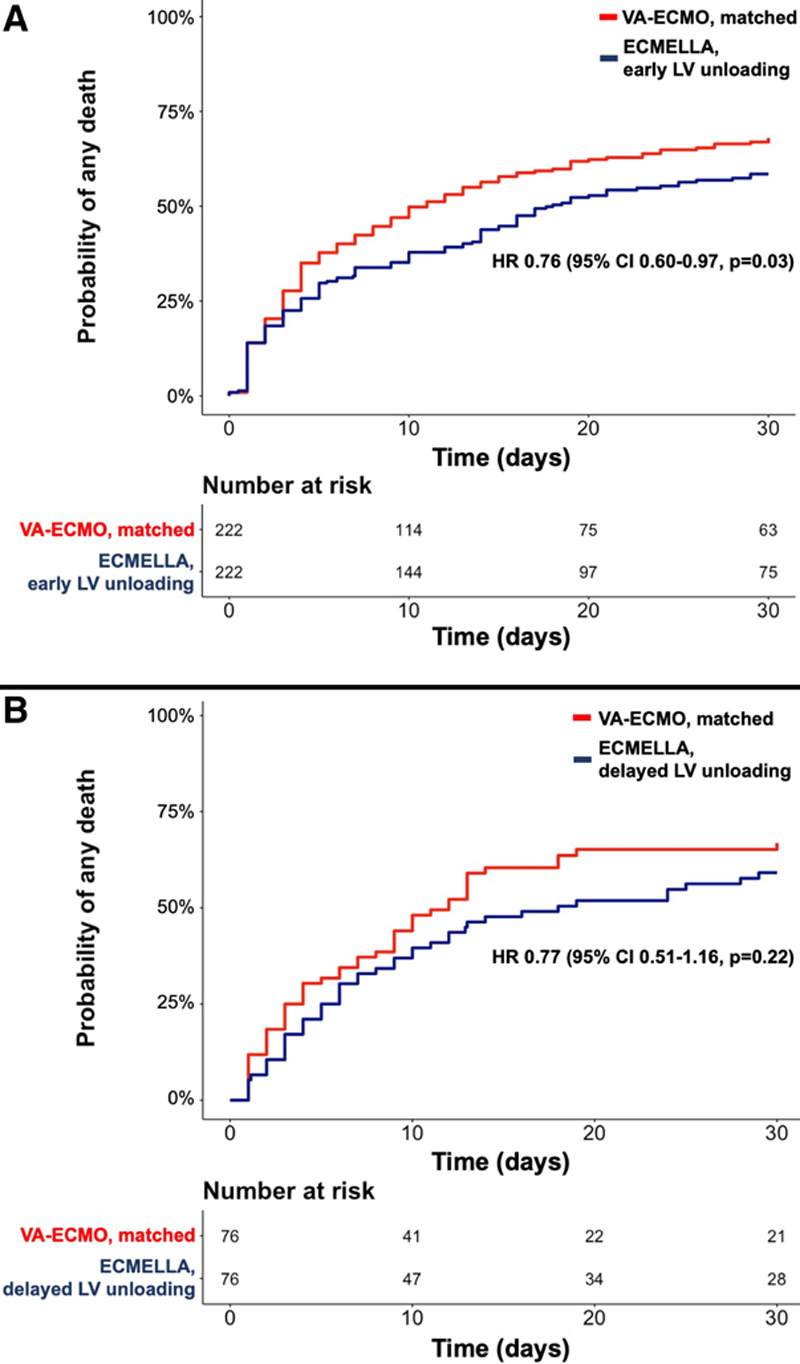
Results: Left ventricular unloading was used in 337 of the 686 patients (49%). After matching, 255 patients with left ventricular unloading were compared with 255 patients without left ventricular unloading. In the matched cohort, left ventricular unloading was associated with lower 30-day mortality (hazard ratio, 0.79 [95% CI, 0.63-0.98]; P=0.03) without differences in various subgroups. Complications occurred more frequently in patients with left ventricular unloading: severe bleeding in 98 (38.4%) versus 45 (17.9%), access site-related ischemia in 55 (21.6%) versus 31 (12.3%), abdominal compartment in 23 (9.4%) versus 9 (3.7%), and renal replacement therapy in 148 (58.5%) versus 99 (39.1%).
Conclusions: In this international, multicenter cohort study, left ventricular unloading was associated with lower mortality in patients with cardiogenic shock treated with VA-ECMO, despite higher complication rates. These findings support use of left ventricular unloading in patients with cardiogenic shock treated with VA-ECMO and call for further validation, ideally in a randomized, controlled trial.
Keywords: extracorporeal membrane oxygenation; shock, cardiogenic.
Figures
Comment in
-
Routine Unloading in Patients Treated With Extracorporeal Membrane Oxygenation for Cardiogenic Shock: Mixed Outcomes Set the Stage for Future Trials.Circulation. 2020 Dec;142(22):2107-2109. doi: 10.1161/CIRCULATIONAHA.120.050847. Epub 2020 Nov 30. Circulation. 2020. PMID: 33252999 No abstract available.
-
Letter by Mehmood Regarding Article, "Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study".Circulation. 2021 Jun 8;143(23):e1021. doi: 10.1161/CIRCULATIONAHA.120.052111. Epub 2021 Jun 7. Circulation. 2021. PMID: 34097445 No abstract available.
-
Response by Schrage and Westermann to Letters Regarding Article, "Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study".Circulation. 2021 Jun 8;143(23):e1024. doi: 10.1161/CIRCULATIONAHA.121.053992. Epub 2021 Jun 7. Circulation. 2021. PMID: 34097447 No abstract available.
-
Letter by Meuwese et al Regarding Article, "Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results From an International, Multicenter Cohort Study".Circulation. 2021 Jun 8;143(23):e1022-e1023. doi: 10.1161/CIRCULATIONAHA.120.053263. Epub 2021 Jun 7. Circulation. 2021. PMID: 34097450 No abstract available.
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, González-Juanatey JR, Harjola VP, Jankowska EA, et al. ; ESC Scientific Document Group. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC): developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128 - PubMed
-
- Becher PM, Schrage B, Sinning CR, Schmack B, Fluschnik N, Schwarzl M, Waldeyer C, Lindner D, Seiffert M, Neumann JT, et al. Venoarterial extracorporeal membrane oxygenation for cardiopulmonary support. Circulation. 2018;138:2298–2300. doi: 10.1161/CIRCULATIONAHA.118.036691 - PubMed
-
- Thiele H, Ohman EM, de Waha-Thiele S, Zeymer U, Desch S. Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur Heart J. 2019;40:2671–2683. doi: 10.1093/eurheartj/ehz363 - PubMed
-
- Brunner S, Guenther SPW, Lackermair K, Peterss S, Orban M, Boulesteix AL, Michel S, Hausleiter J, Massberg S, Hagl C. Extracorporeal life support in cardiogenic shock complicating acute myocardial infarction. J Am Coll Cardiol. 2019;73:2355–2357. doi: 10.1016/j.jacc.2019.02.044 - PubMed
-
- Schrage B, Burkhoff D, Rübsamen N, Becher PM, Schwarzl M, Bernhardt A, Grahn H, Lubos E, Söffker G, Clemmensen P, et al. Unloading of the left ventricle during venoarterial extracorporeal membrane oxygenation therapy in cardiogenic shock. JACC Heart Fail. 2018;6:1035–1043. doi: 10.1016/j.jchf.2018.09.009 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
