

The impact of dementia and language on hospitalizations: a retrospective cohort of long-term care residents
- PMID: 33032528
- PMCID: PMC7545542
- DOI: 10.1186/s12877-020-01806-2
The impact of dementia and language on hospitalizations: a retrospective cohort of long-term care residents
Abstract
Background: Hospitalizations carry considerable risks for frail, elderly patients; this is especially true for patients with dementia, who are more likely to experience delirium, falls, functional decline, iatrogenic complications, and infections when compared to their peers without dementia. Since up to two thirds of patients in long-term care (LTC) facilities have dementia, there is interest in identifying factors associated with transitions from LTC facilities to hospitals. The purpose of this study was to investigate the association between dementia status and incidence of hospitalization among residents in LTC facilities in Ontario, Canada, and to determine whether this association is modified by linguistic factors.
Methods: We used linked administrative databases to establish a prevalent cohort of 81,188 residents in 628 LTC facilities from April 1st 2014 to March 31, 2017. Diagnoses of dementia were identified with a previously validated algorithm; all other patient characteristics were obtained from in-person assessments. Residents' primary language was coded as English or French; facility language (English or French) was determined using language designation status according to the French Language Services Act. We identified all hospitalizations within 3 months of the first assessment performed after April 1st 2014. We performed multivariate logistic regression analyses to determine the impact of dementia and resident language on the incidence of hospitalization; we also considered interactions between dementia and both resident language and resident-facility language discordance.
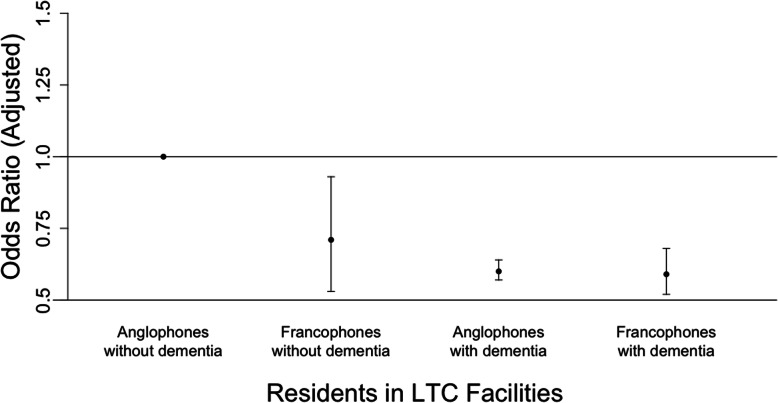
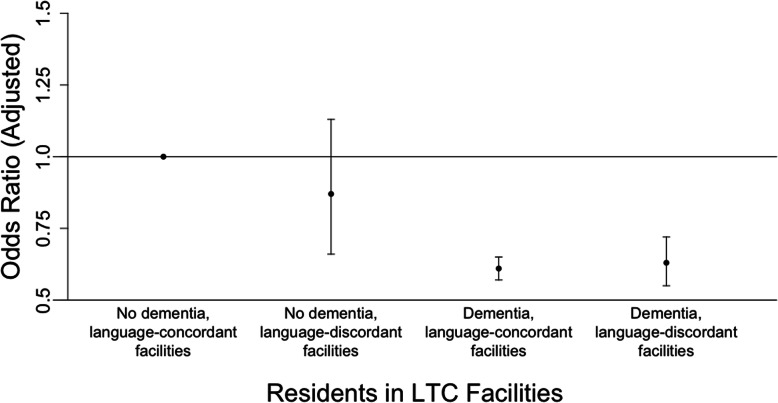
Results: The odds of hospitalization were 39% lower for residents with dementia compared to residents without dementia (OR 0.61, 95% CI 0.57-0.65). Francophones had lower odds of hospitalization than Anglophones, but this difference was not statistically significant (OR 0.91, 95% CI 0.81-1.03). However, Francophones without dementia were significantly less likely to be hospitalized compared to Anglophones without dementia (OR 0.71, 95% CI 0.53-0.94). Resident-facility language discordance did not significantly affect hospitalizations.
Conclusions: Residents in LTC facilities were generally less likely to be hospitalized if they had dementia, or if their primary language was French and they did not have dementia. These findings could be explained by differences in end-of-life care goals; however, they could also be the result of poor patient-provider communication.
Keywords: Dementia; Hospitalizations; Language; Long-term care; Nursing homes.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization . Dementia. 2020.
-
- Canadian Institute for Health Information . Continuing Care Reporting System: Data Users Guide. 2020.
-
- Sloane PD, Zimmerman S, Gruber-Baldini AL, Hebel JR, Magaziner J, Konrad TR. Health and functional outcomes and health care utilization of persons with dementia in residential care and assisted living facilities: comparison with nursing homes. The Gerontologist. 2005;45(suppl):124–134. doi: 10.1093/geront/45.suppl_1.124. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
