

Ketamine-propofol (Ketofol) for procedural sedation and analgesia in children: a systematic review and meta-analysis
- PMID: 33032544
- PMCID: PMC7545911
- DOI: 10.1186/s12873-020-00373-4
Ketamine-propofol (Ketofol) for procedural sedation and analgesia in children: a systematic review and meta-analysis
Abstract
Objectives: The aim of this review is to elucidate the efficacy and side effects of ketofol in comparison to other anaesthetic agents during procedural sedation and analgesia.
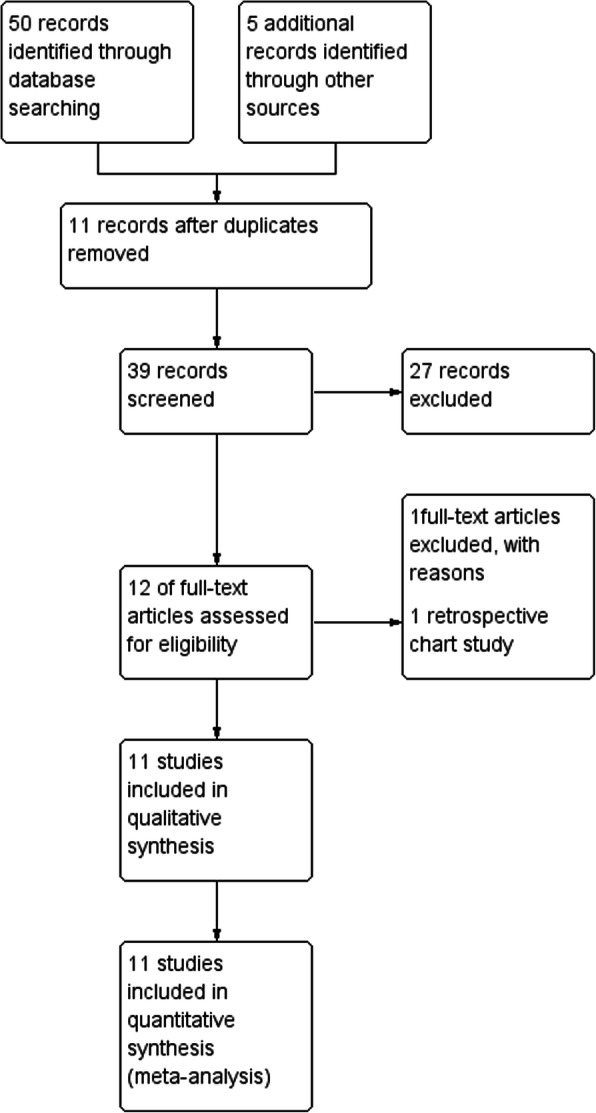
Method: The Cochrane Central Register of Controlled Trials (1996 to Feb 2019) and MEDLINE (1966 to Feb 2019) were searched, including the related randomised control trials and reviewed articles to find unpublished trials or trials not obtained via electronic searches. Inclusion criteria for the studies included comparing recovery time, recording clinician satisfaction, and assessing the adverse effects of ketofol.
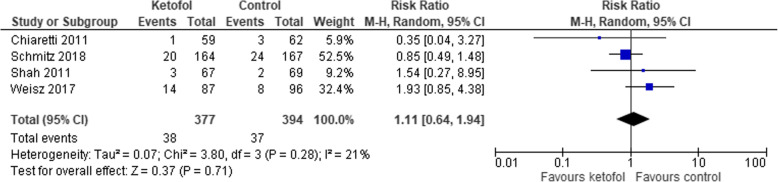
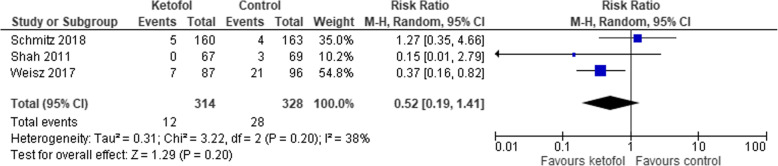
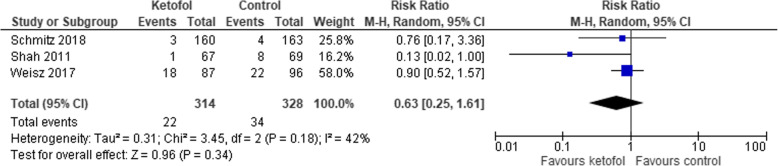
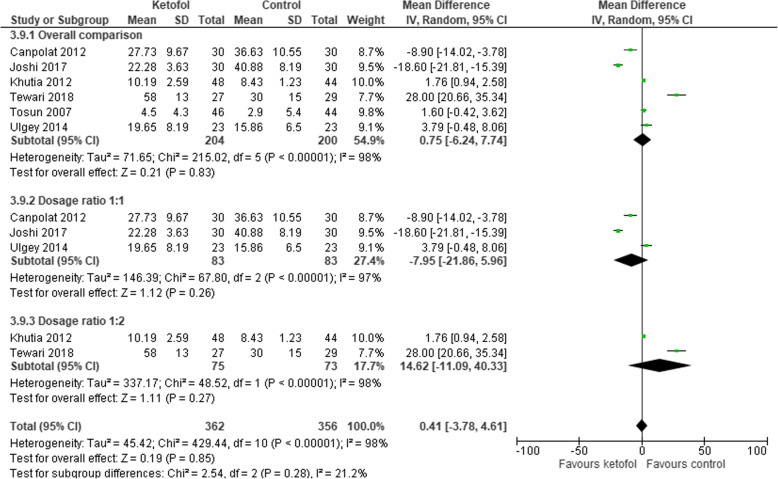
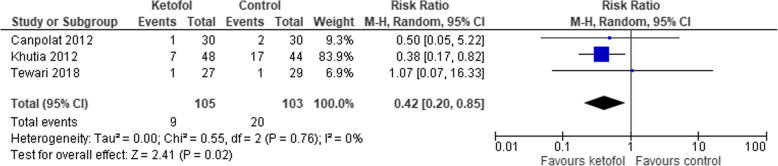
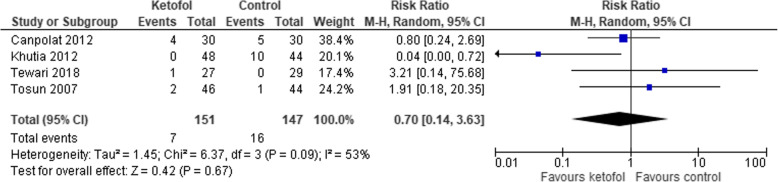
Results: Eleven trials consisting of a total of 1274 patients met our criteria and were included in this meta-analysis. Five trials compared ketofol with a single agent, while six trials compared ketofol with combined agents. While comparing between ketofol and a single agent (either ketamine or propofol), ketofol showed significant effect on recovery time (MD: -9.88, 95% CI: - 14.30 to - 5.46; P = 0.0003; I2 = 92%). However, no significant difference was observed while comparing ketofol with combined agents (RR: 0.75, 95% CI: - 6.24 to 7.74; P < 0.001; I2 = 98%). During single-agent comparison, ketofol showed no significant differences in terms of clinician satisfaction (RR: 2.86, 95% CI: 0.64 to 12.69; P = 0.001; I2 = 90%), airway obstruction (RR: 0.72, 95% CI: 0.35 to 11.48; P = 0.81; I2 = 0%), apnoea (RR: 0.9, 95% CI: 0.33 to 2.44; P = 0.88; I2 = 0%), desaturation (RR: 1.11, 95% CI: 0.64 to 1.94; P = 0.28; I2 = 21%), nausea (RR: 0.52, 95% CI: 0.91 to 1.41; P = 0.2; I2 = 38%), and vomiting (RR: 0.63, 95% CI: 0.25 to 1.61; P = 0.18; I2 = 42%). During comparison with combined agents, ketofol was more effective in reducing hypotension (RR: 4.2, 95% CI: 0.2 to 0.85; P = 0.76; I2 = 0%), but no differences were observed in terms of bradycardia (RR: 0.70, 95% CI: 0.14 to 03.63; P = 0.09; I2 = 53%), desaturation (RR: 1.9, 95% CI: 0.15 to 23.6; P = 0.11; I2 = 61%), and respiratory depression (RR: 1.98, 95% CI: 0.18 to 21.94; P = 0.12; I2 = 59%).
Conclusion: There is low certainty of evidence that ketofol improves recovery time and moderate certainty of evidence that it reduces the frequency of hypotension. There was no significant difference in terms of other adverse effects when compared to other either single or combined agents.
Trial registration: PROSPERO CRD42019127278 .
Keywords: Children; Ketamine-propofol; Ketofol; Meta-analysis; Paediatric; Procedural sedation and analgesia; Systematic review.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures






References
-
- Godwin SA, Burton JH, Gerardo CJ, et al. Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department. Ann Emerg Med. 2014;63(2):247–258.e218. - PubMed
-
- Chawla N, Boateng A, Deshpande R. Procedural sedation in the ICU and emergency department. Curr Opin Anaesthesiol. 2017;30(4):507–512. - PubMed
-
- Krieser D, Kochar A. Paediatric procedural sedation within the emergency department. J Paediatr Child Health. 2016;52(2):197–203. - PubMed
-
- Eberson CP, Hsu RY, Borenstein TR. Procedural sedation in the emergency department. J Am Acad Orthop Surg. 2015;23(4):233–242. - PubMed
-
- Jalili M, Bahreini M, Doosti-Irani A, Masoomi R, Arbab M, Mirfazaelian H. Ketamine-propofol combination (ketofol) vs propofol for procedural sedation and analgesia: systematic review and meta-analysis. Am J Emerg Med. 2016;34(3):558–569. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
