

Impact of hematologic malignancy and type of cancer therapy on COVID-19 severity and mortality: lessons from a large population-based registry study
- PMID: 33032660
- PMCID: PMC7542567
- DOI: 10.1186/s13045-020-00970-7
Impact of hematologic malignancy and type of cancer therapy on COVID-19 severity and mortality: lessons from a large population-based registry study
Abstract
Background: Patients with cancer have been shown to have a higher risk of clinical severity and mortality compared to non-cancer patients with COVID-19. Patients with hematologic malignancies typically are known to have higher levels of immunosuppression and may develop more severe respiratory viral infections than patients with solid tumors. Data on COVID-19 in patients with hematologic malignancies are limited. Here we characterize disease severity and mortality and evaluate potential prognostic factors for mortality.
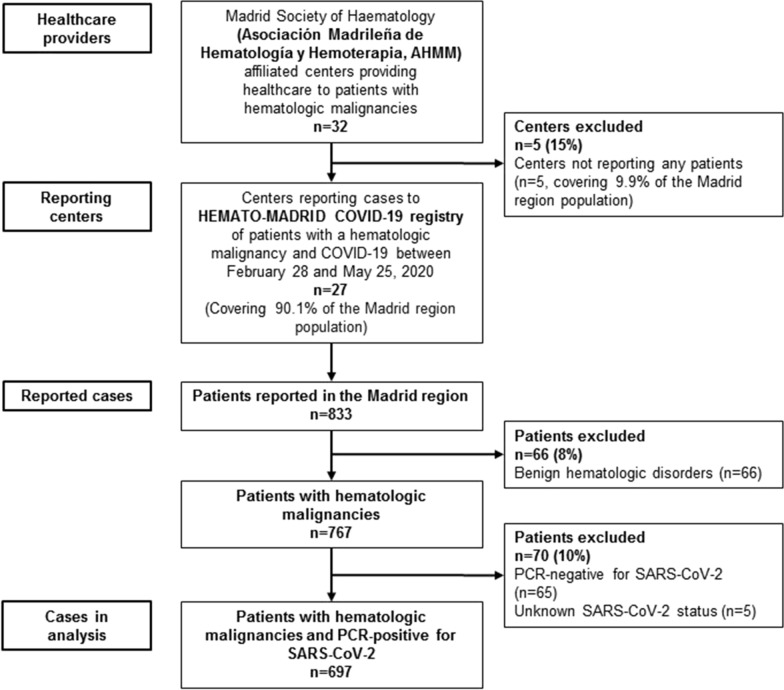
Methods: In this population-based registry study, we collected de-identified data on clinical characteristics, treatment and outcomes in adult patients with hematologic malignancies and confirmed severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection within the Madrid region of Spain. Our case series included all patients admitted to 22 regional health service hospitals and 5 private healthcare centers between February 28 and May 25, 2020. The primary study outcome was all-cause mortality. We assessed the association between mortality and potential prognostic factors using Cox regression analyses adjusted for age, sex, comorbidities, hematologic malignancy and recent active cancer therapy.
Results: Of 833 patients reported, 697 were included in the analyses. Median age was 72 years (IQR 60-79), 413 (60%) patients were male and 479 (69%) and 218 (31%) had lymphoid and myeloid malignancies, respectively. Clinical severity of COVID-19 was severe/critical in 429 (62%) patients. At data cutoff, 230 (33%) patients had died. Age ≥ 60 years (hazard ratios 3.17-10.1 vs < 50 years), > 2 comorbidities (1.41 vs ≤ 2), acute myeloid leukemia (2.22 vs non-Hodgkin lymphoma) and active antineoplastic treatment with monoclonal antibodies (2·02) were associated with increased mortality; conventional chemotherapy showed borderline significance (1.50 vs no active therapy). Conversely, Ph-negative myeloproliferative neoplasms (0.33) and active treatment with hypomethylating agents (0.47) were associated with lower mortality. Overall, 574 (82%) patients received antiviral therapy. Mortality with severe/critical COVID-19 was higher with no therapy vs any antiviral combination therapy (2.20).
Conclusions: In this series of patients with hematologic malignancies and COVID-19, mortality was associated with higher age, more comorbidities, type of hematological malignancy and type of antineoplastic therapy. Further studies and long-term follow-up are required to validate these criteria for risk stratification.
Keywords: COVID-19; Hematologic neoplasms; Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Timeline of WHO’s response to COVID-19. 2020 15/07/2020. https://www.who.int/news-room/detail/29-06-2020-covidtimeline.
-
- European Centre for Disease Prevention and Control. COVID-19 situation update worldwide. 2020 15/07/2020. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
