

Impact of Public Health Emergency Response to COVID-19 on Management and Outcome for STEMI Patients in Beijing-A Single-Center Historic Control Study
- PMID: 33032817
- PMCID: PMC7462598
- DOI: 10.1016/j.cpcardiol.2020.100693
Impact of Public Health Emergency Response to COVID-19 on Management and Outcome for STEMI Patients in Beijing-A Single-Center Historic Control Study
Abstract
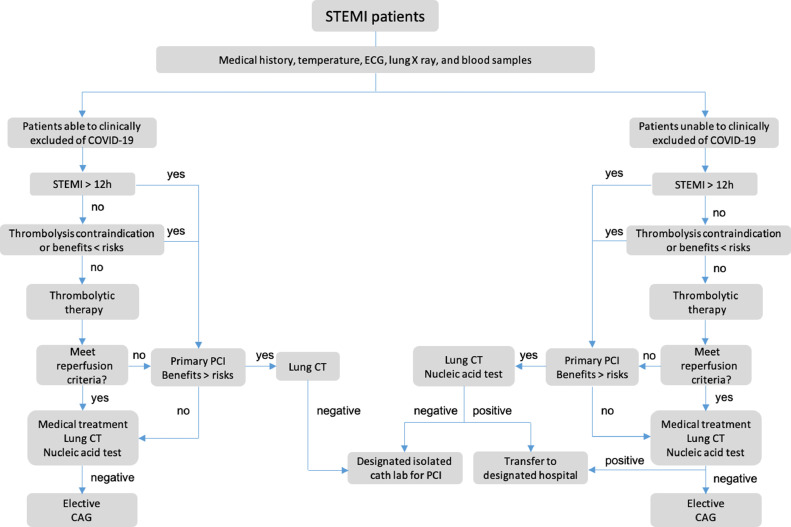
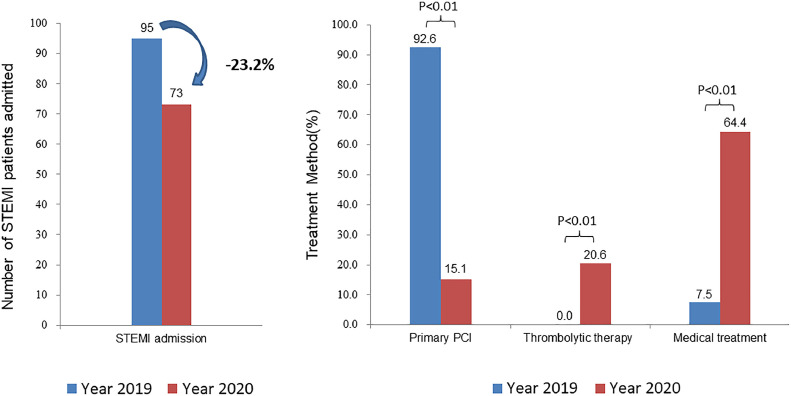
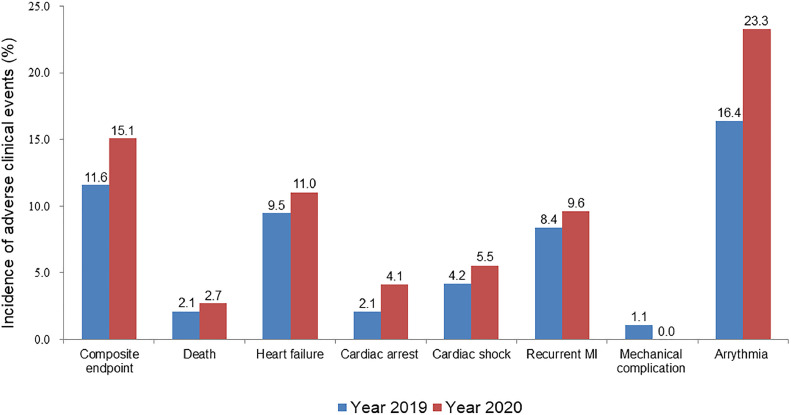
Coronavirus disease 2019 (COVID-19) pandemic poses great challenge on public health globally. To clarify the impact of COVID-19 pandemic on in-hospital management and outcomes for ST-segment elevation myocardial infarction (STEMI) patients in the nonepicenter. We enrolled consecutive STEMI patients who visited Fuwai Hospital from January to March, 2020 (N = 73) and also established a historical control including all consecutive STEMI patients in the same period of 2019 (N = 95). The primary outcome was defined as a composite endpoint of all-cause death, heart failure, cardiac shock, and cardiac arrest during hospitalization. Emergency response for COVID-19 resulted in a significant 77.6% reduction in the number of primary percutaneous coronary intervention, and a trend toward higher rate of primary composite endpoint (15.1% vs 11.6%, P = 0.51). COVID-19 pandemic results in a significant reduction in emergent reperfusion therapy, and a trend toward higher in-hospital adverse events risk.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed July 15, 2020.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
