

Utilization of Deep Learning for Subphenotype Identification in Sepsis-Associated Acute Kidney Injury
- PMID: 33033164
- PMCID: PMC7646246
- DOI: 10.2215/CJN.09330819
Utilization of Deep Learning for Subphenotype Identification in Sepsis-Associated Acute Kidney Injury
Abstract
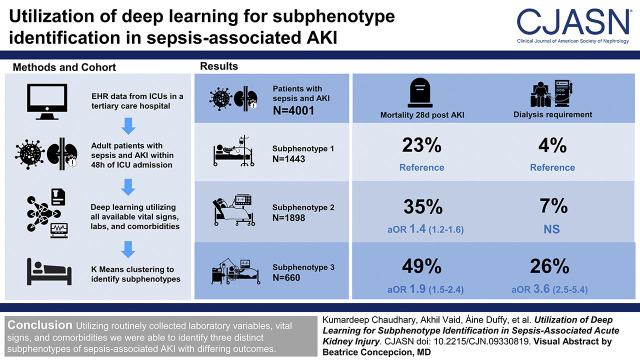
Background and objectives: Sepsis-associated AKI is a heterogeneous clinical entity. We aimed to agnostically identify sepsis-associated AKI subphenotypes using deep learning on routinely collected data in electronic health records.
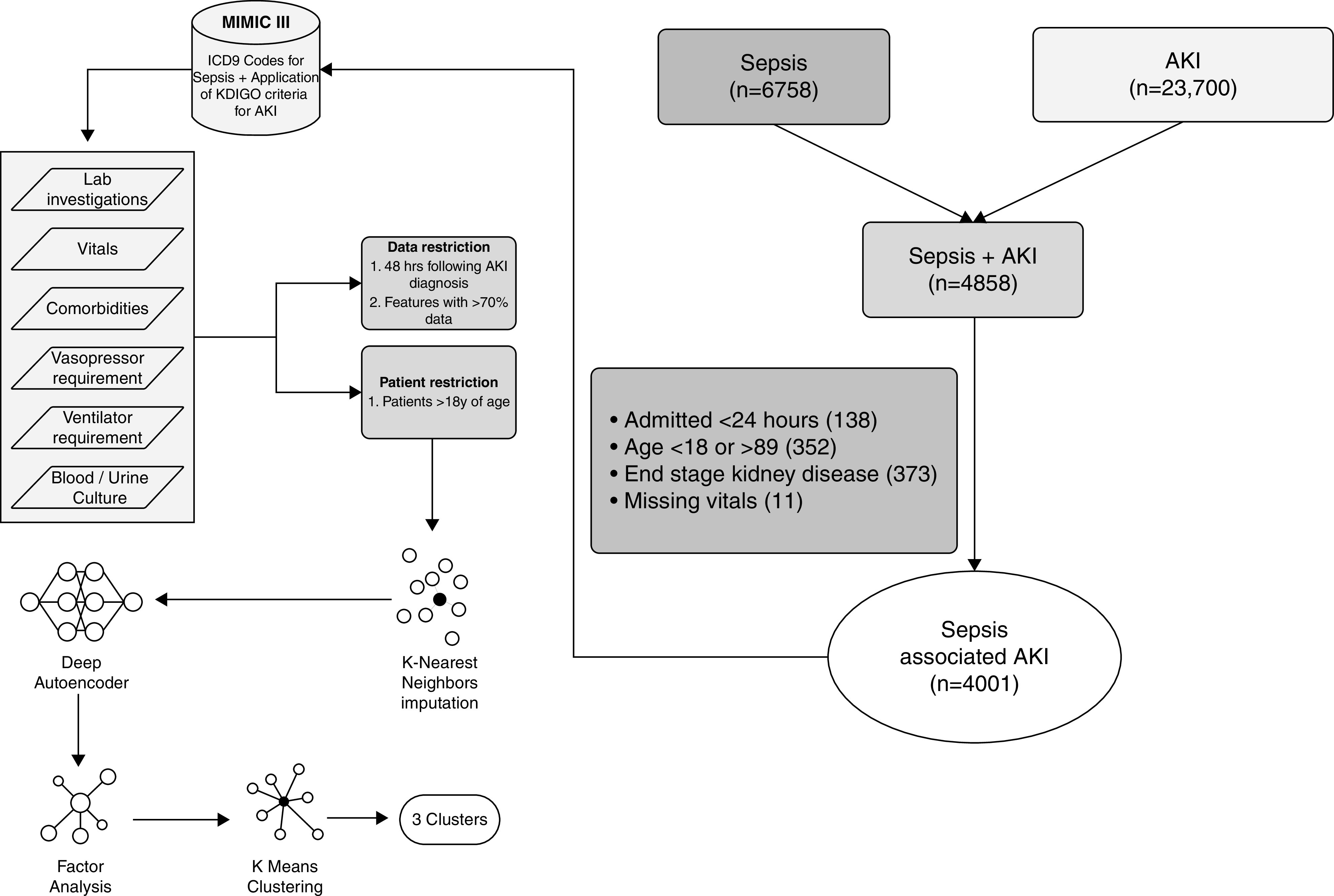
Design, setting, participants, & measurements: We used the Medical Information Mart for Intensive Care III database, which consists of electronic health record data from intensive care units in a tertiary care hospital in the United States. We included patients ≥18 years with sepsis who developed AKI within 48 hours of intensive care unit admission. We then used deep learning to utilize all available vital signs, laboratory measurements, and comorbidities to identify subphenotypes. Outcomes were mortality 28 days after AKI and dialysis requirement.
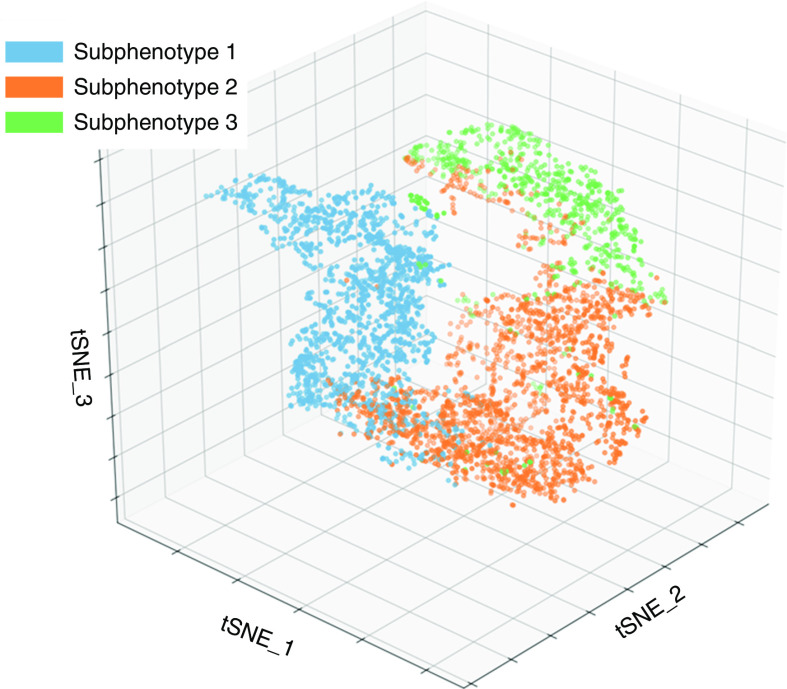
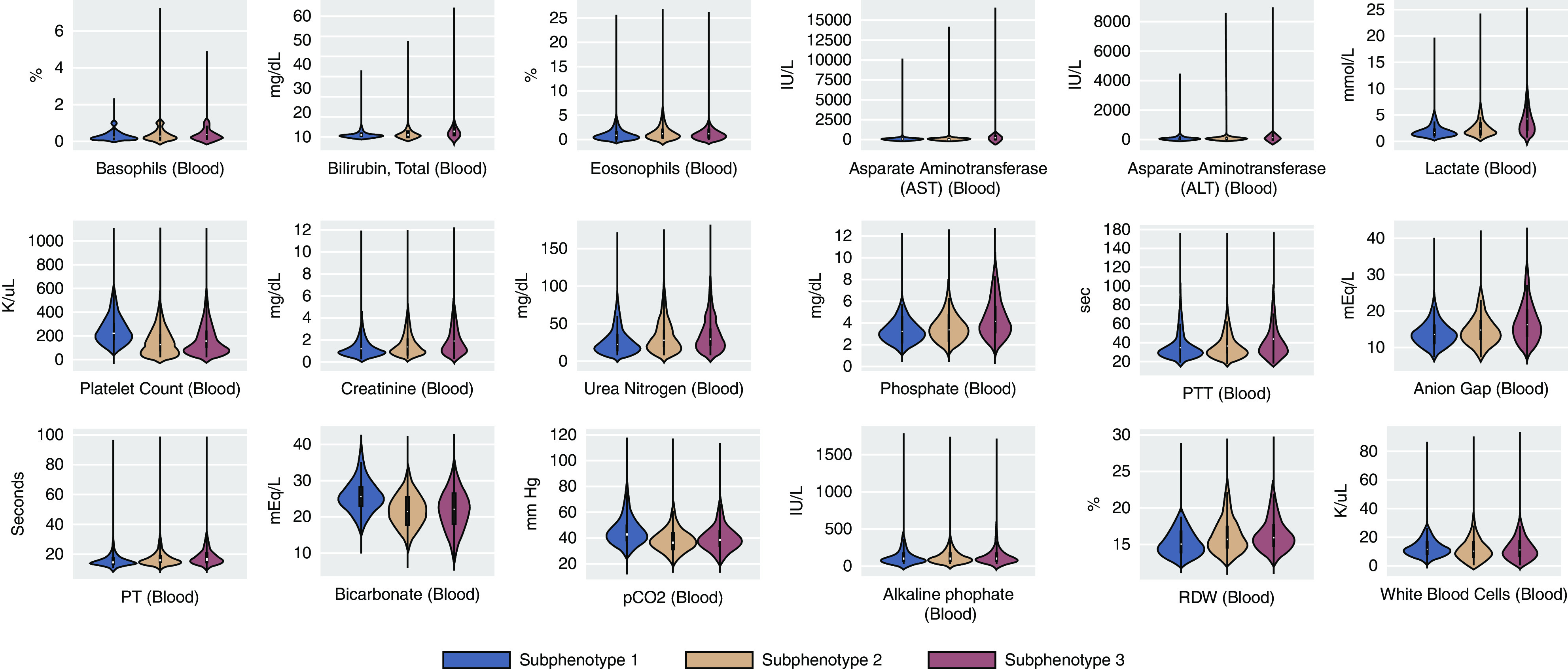
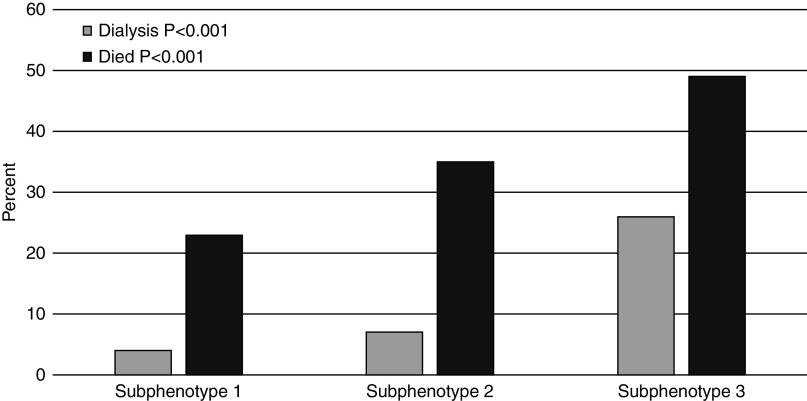
Results: We identified 4001 patients with sepsis-associated AKI. We utilized 2546 combined features for K-means clustering, identifying three subphenotypes. Subphenotype 1 had 1443 patients, and subphenotype 2 had 1898 patients, whereas subphenotype 3 had 660 patients. Subphenotype 1 had the lowest proportion of liver disease and lowest Simplified Acute Physiology Score II scores compared with subphenotypes 2 and 3. The proportions of patients with CKD were similar between subphenotypes 1 and 3 (15%) but highest in subphenotype 2 (21%). Subphenotype 1 had lower median bilirubin levels, aspartate aminotransferase, and alanine aminotransferase compared with subphenotypes 2 and 3. Patients in subphenotype 1 also had lower median lactate, lactate dehydrogenase, and white blood cell count than patients in subphenotypes 2 and 3. Subphenotype 1 also had lower creatinine and BUN than subphenotypes 2 and 3. Dialysis requirement was lowest in subphenotype 1 (4% versus 7% [subphenotype 2] versus 26% [subphenotype 3]). The mortality 28 days after AKI was lowest in subphenotype 1 (23% versus 35% [subphenotype 2] versus 49% [subphenotype 3]). After adjustment, the adjusted odds ratio for mortality for subphenotype 3, with subphenotype 1 as a reference, was 1.9 (95% confidence interval, 1.5 to 2.4).
Conclusions: Utilizing routinely collected laboratory variables, vital signs, and comorbidities, we were able to identify three distinct subphenotypes of sepsis-associated AKI with differing outcomes.
Keywords: AKI; acute kidney injury; acute renal failure; deep learning; dialysis; mortality; subtypes.
Copyright © 2020 by the American Society of Nephrology.
Figures
Comment in
-
Not All Sepsis-Associated Acute Kidney Injury Is the Same: There May Be an App for That.Clin J Am Soc Nephrol. 2020 Nov 6;15(11):1543-1545. doi: 10.2215/CJN.14860920. Epub 2020 Oct 8. Clin J Am Soc Nephrol. 2020. PMID: 33034570 Free PMC article. No abstract available.
Similar articles
-
Acute kidney injury subphenotypes based on creatinine trajectory identifies patients at increased risk of death.Crit Care. 2016 Nov 17;20(1):372. doi: 10.1186/s13054-016-1546-4. Crit Care. 2016. PMID: 27852290 Free PMC article.
-
Two subphenotypes of septic acute kidney injury are associated with different 90-day mortality and renal recovery.Crit Care. 2020 Apr 15;24(1):150. doi: 10.1186/s13054-020-02866-x. Crit Care. 2020. PMID: 32295614 Free PMC article.
-
IDENTIFICATION OF SUBPHENOTYPES OF SEPSIS-ASSOCIATED LIVER DYSFUNCTION USING CLUSTER ANALYSIS.Shock. 2023 Mar 1;59(3):368-374. doi: 10.1097/SHK.0000000000002068. Epub 2022 Dec 23. Shock. 2023. PMID: 36562264
-
Defining phenotypes and treatment effect heterogeneity to inform acute respiratory distress syndrome and sepsis trials: secondary analyses of three RCTs.Southampton (UK): NIHR Journals Library; 2021 Jul. Southampton (UK): NIHR Journals Library; 2021 Jul. PMID: 34347404 Free Books & Documents. Review.
-
Using Predictive Models to Improve Care for Patients Hospitalized with COVID-19 [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2023 Jan. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2023 Jan. PMID: 38976624 Free Books & Documents. Review.
Cited by
-
[Artificial intelligence and acute kidney injury].Med Klin Intensivmed Notfmed. 2024 Apr;119(3):199-207. doi: 10.1007/s00063-024-01111-5. Epub 2024 Feb 23. Med Klin Intensivmed Notfmed. 2024. PMID: 38396124 Free PMC article. Review. German.
-
Sub-Phenotypes of Acute Kidney Injury: Do We Have Progress for Personalizing Care?Nephron. 2020;144(12):677-679. doi: 10.1159/000511321. Epub 2020 Oct 22. Nephron. 2020. PMID: 33091901 Free PMC article. Review.
-
Machine learning for early discrimination between transient and persistent acute kidney injury in critically ill patients with sepsis.Sci Rep. 2021 Oct 12;11(1):20269. doi: 10.1038/s41598-021-99840-6. Sci Rep. 2021. PMID: 34642418 Free PMC article.
-
Application of Machine Learning for Clinical Subphenotype Identification in Sepsis.Infect Dis Ther. 2022 Oct;11(5):1949-1964. doi: 10.1007/s40121-022-00684-y. Epub 2022 Aug 25. Infect Dis Ther. 2022. PMID: 36006560 Free PMC article.
-
A novel method leveraging time series data to improve subphenotyping and application in critically ill patients with COVID-19.Artif Intell Med. 2024 Feb;148:102750. doi: 10.1016/j.artmed.2023.102750. Epub 2023 Dec 20. Artif Intell Med. 2024. PMID: 38325922 Free PMC article.
References
-
- Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J: Independent association between acute renal failure and mortality following cardiac surgery. Am J Med 104: 343–348, 1998. - PubMed
-
- de Mendonça A, Vincent JL, Suter PM, Moreno R, Dearden NM, Antonelli M, Takala J, Sprung C, Cantraine F: Acute renal failure in the ICU: Risk factors and outcome evaluated by the SOFA score. Intensive Care Med 26: 915–921, 2000. - PubMed
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW: Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 16: 3365–3370, 2005. - PubMed
-
- Prowle JR, Ishikawa K, May CN, Bellomo R: Renal blood flow during acute renal failure in man. Blood Purif 28: 216–225, 2009. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
