

SARS-CoV-2 exposure, symptoms and seroprevalence in healthcare workers in Sweden
- PMID: 33033249
- PMCID: PMC7544689
- DOI: 10.1038/s41467-020-18848-0
SARS-CoV-2 exposure, symptoms and seroprevalence in healthcare workers in Sweden
Abstract
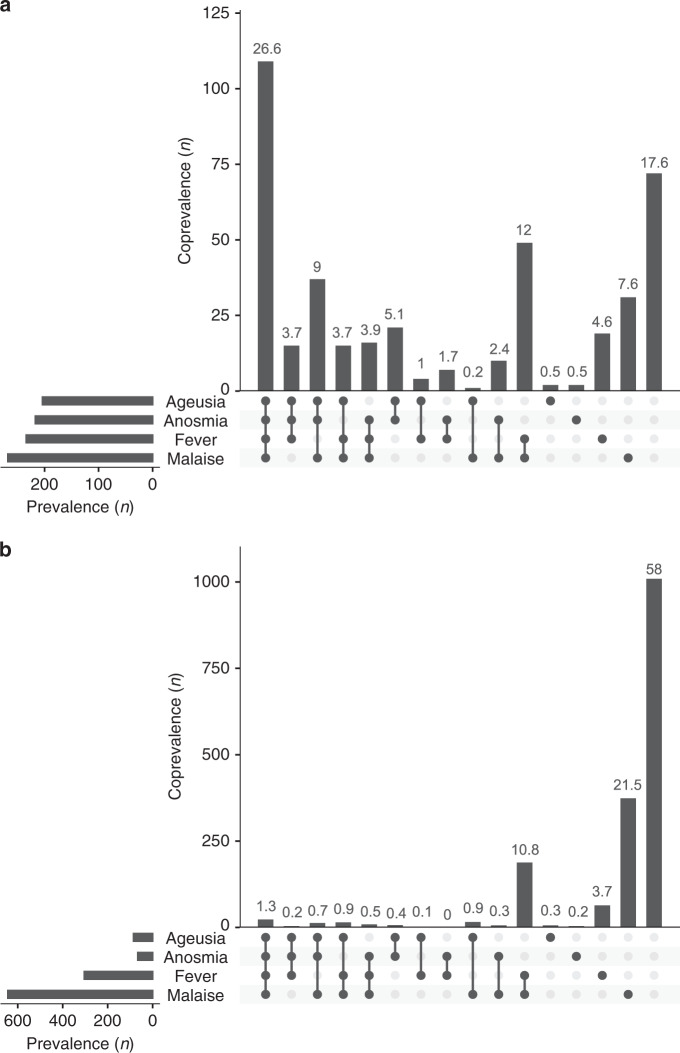
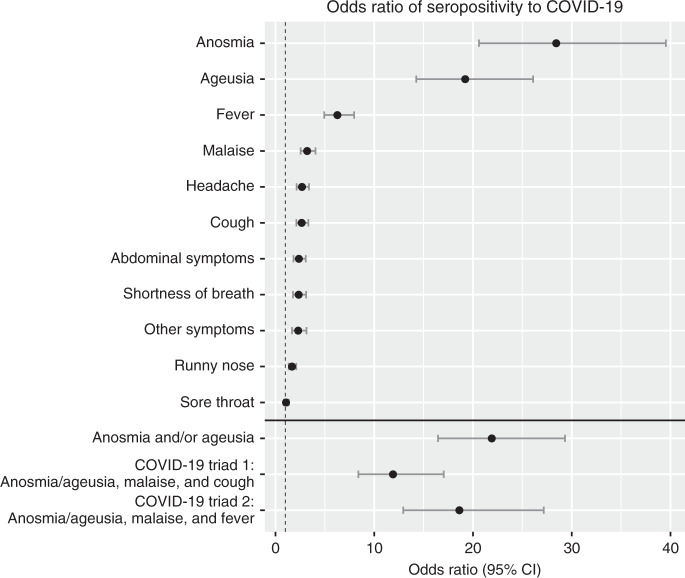
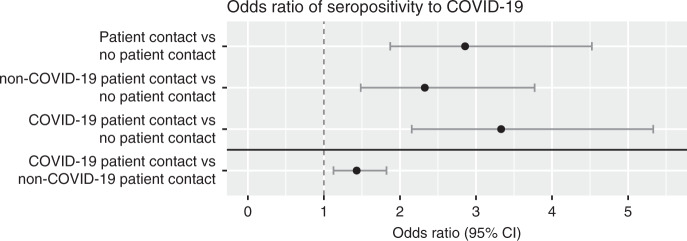
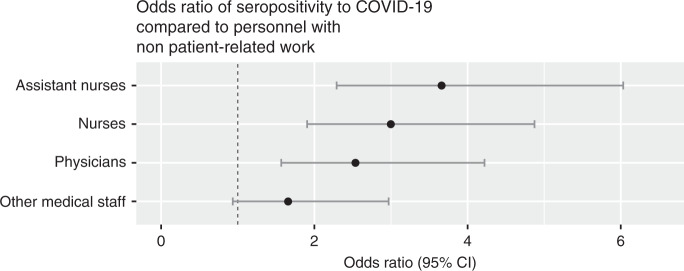
SARS-CoV-2 may pose an occupational health risk to healthcare workers. Here, we report the seroprevalence of SARS-CoV-2 antibodies, self-reported symptoms and occupational exposure to SARS-CoV-2 among healthcare workers at a large acute care hospital in Sweden. The seroprevalence of IgG antibodies against SARS-CoV-2 was 19.1% among the 2149 healthcare workers recruited between April 14th and May 8th 2020, which was higher than the reported regional seroprevalence during the same time period. Symptoms associated with seroprevalence were anosmia (odds ratio (OR) 28.4, 95% CI 20.6-39.5) and ageusia (OR 19.2, 95% CI 14.3-26.1). Seroprevalence was also associated with patient contact (OR 2.9, 95% CI 1.9-4.5) and covid-19 patient contact (OR 3.3, 95% CI 2.2-5.3). These findings imply an occupational risk for SARS-CoV-2 infection among healthcare workers. Continued measures are warranted to assure healthcare workers safety and reduce transmission from healthcare workers to patients and to the community.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Organization WH. Coronavirus disease 2019 (COVID-19): situation report-63. https://www.who.int/docs/default-source/coronaviruse/situation-reports/2... (2020)
-
- Folkhälsomyndigheten. https://www.folkhalsomyndigheten.se/smittskydd-beredskap/utbrott/aktuell... (2020)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
