

Efficacy and safety of newer P2Y12 inhibitors for acute coronary syndrome: a network meta-analysis
- PMID: 33033323
- PMCID: PMC7545197
- DOI: 10.1038/s41598-020-73871-x
Efficacy and safety of newer P2Y12 inhibitors for acute coronary syndrome: a network meta-analysis
Abstract
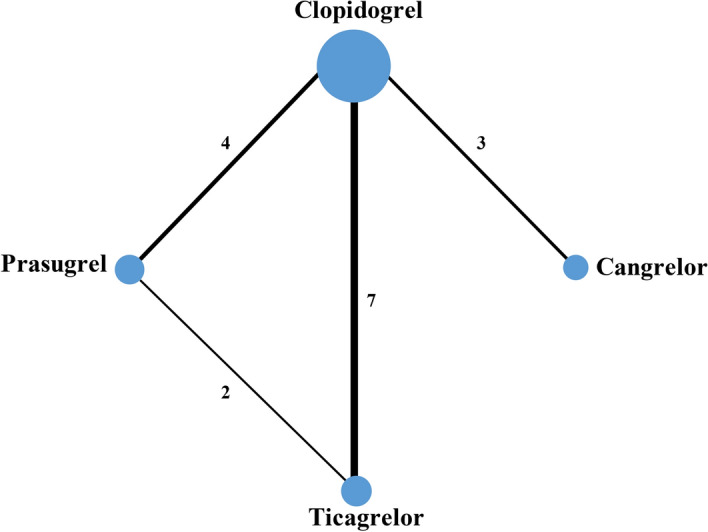
Whether newer P2Y12 inhibitors are more efficacious and safer than clopidogrel and whether there is a superior one remain uncertain. We compared the effect of P2Y12 inhibitors on clinical outcomes in patients with acute coronary syndrome (ACS). Randomized controlled trials comparing clopidogrel, prasugrel, ticagrelor, or cangrelor, in combination with aspirin were searched. Sixteen trials with altogether 77,896 patients were included. Compared to clopidogrel, cardiovascular mortality was reduced with prasugrel (OR 0.85, 95% CI 0.75-0.97) and ticagrelor (0.82, 0.73-0.93). Myocardial infarction (0.75, 0.63-0.89) and major adverse cardiovascular events (0.80, 0.69-0.94) were reduced by prasugrel. Stent thrombosis was reduced by prasugrel (0.49, 0.38-0.63), ticagrelor (0.72, 0.57-0.90), and cangrelor (0.59, 0.43-0.81). It was reduced more by prasugrel than ticagrelor (0.69, 0.51-0.93). There were more major bleeds with prasugrel (1.24, 1.05-1.48). Thrombolysis in Myocardial Infarction (TIMI) major bleeding was increased with prasugrel compared to clopidogrel (1.36, 1.11-1.66) and ticagrelor (1.33, 1.06-1.67). TIMI minor bleeding was increased with prasugrel (1.44, 1.16-1.77) and cangrelor (1.47, 1.01-2.16) compared to clopidogrel while it was increased with prasugrel compared to ticagrelor (1.32, 1.01-1.72). Prasugrel is preferable to those ACS patients at low bleeding risk to reduce cardiovascular events whereas ticagrelor is a relatively safe antiplatelet drug of choice for most patients.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Amsterdam EA, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014;64(24):e139–e228. doi: 10.1016/j.jacc.2014.09.017. - DOI - PubMed
-
- O’Gara PT, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e362–425. doi: 10.1161/CIR.0b013e3182742c84. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
