

Nomograms predicting Overall Survival and Cancer-specific Survival for Synchronous Colorectal Liver-limited Metastasis
- PMID: 33033504
- PMCID: PMC7532510
- DOI: 10.7150/jca.46155
Nomograms predicting Overall Survival and Cancer-specific Survival for Synchronous Colorectal Liver-limited Metastasis
Abstract
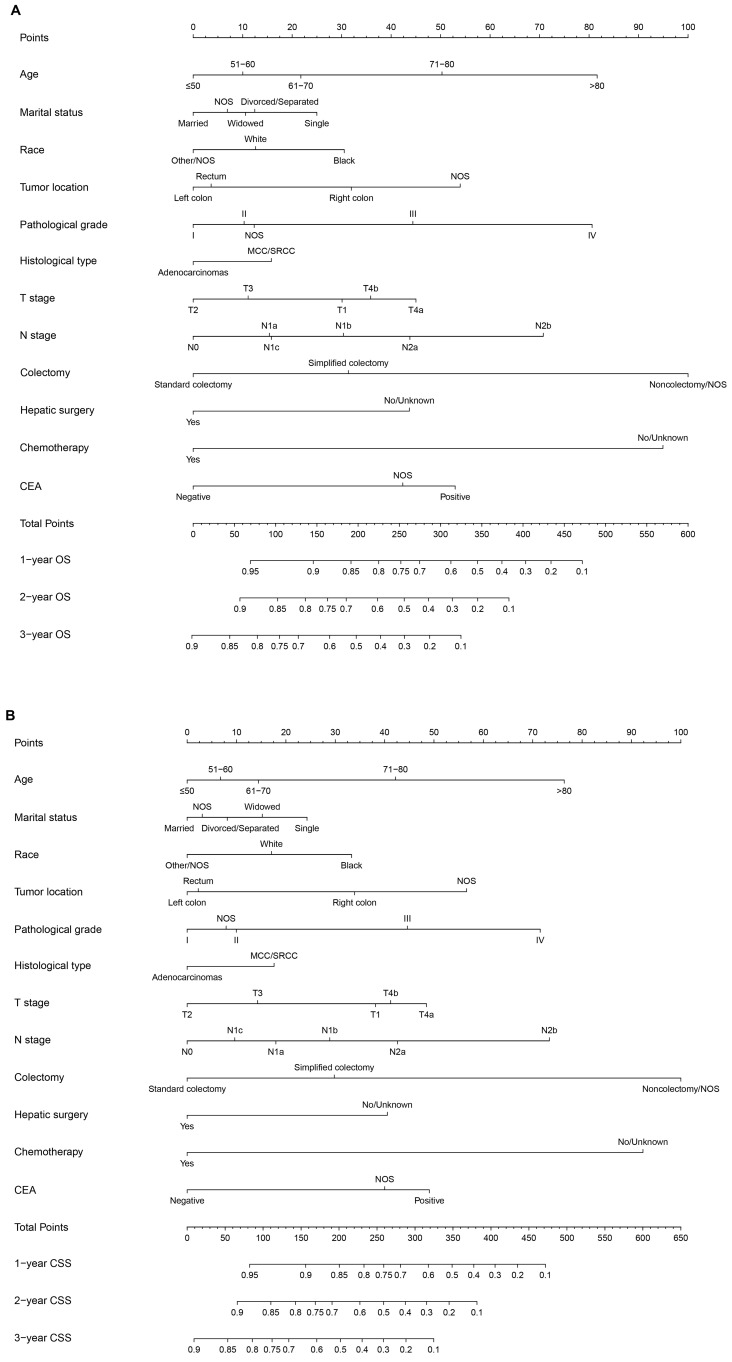
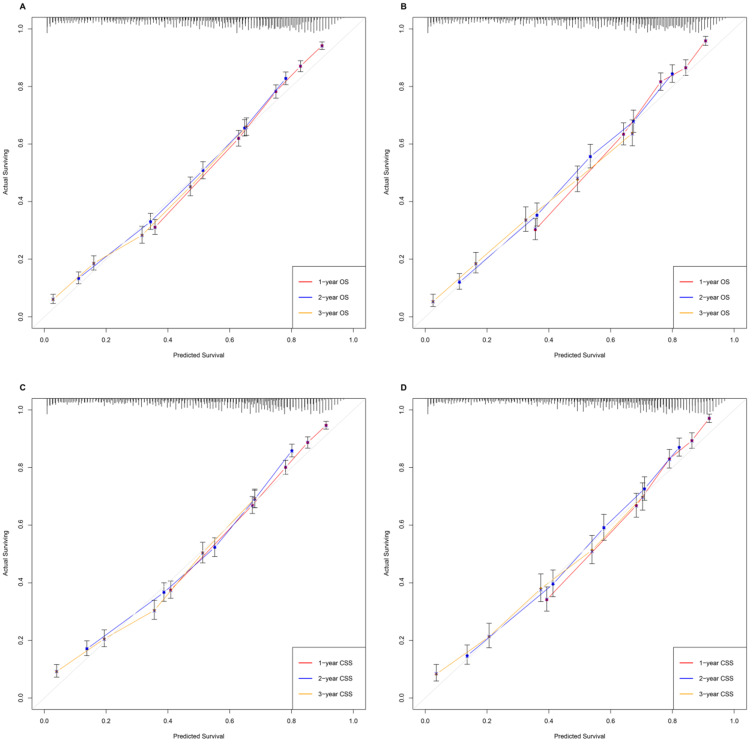
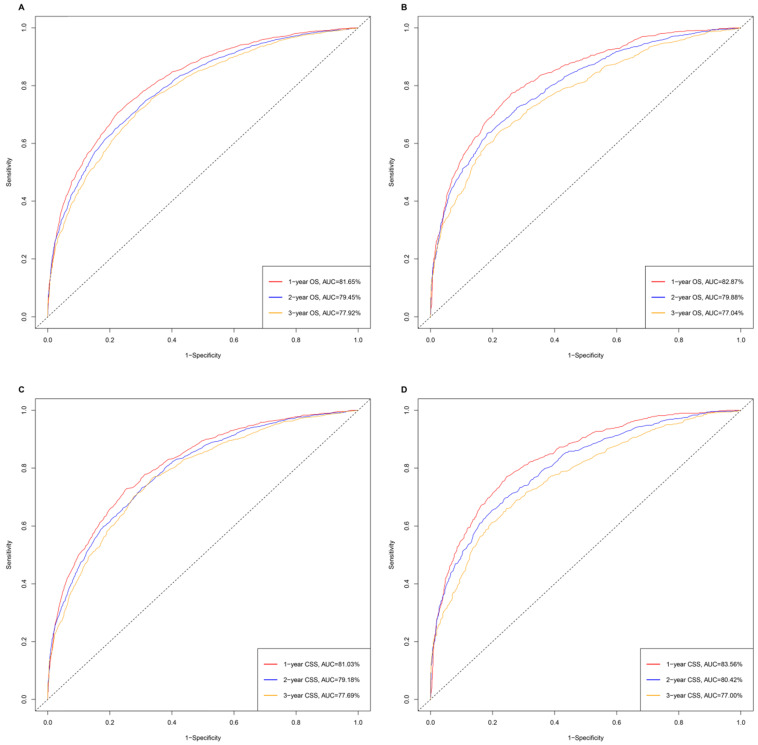
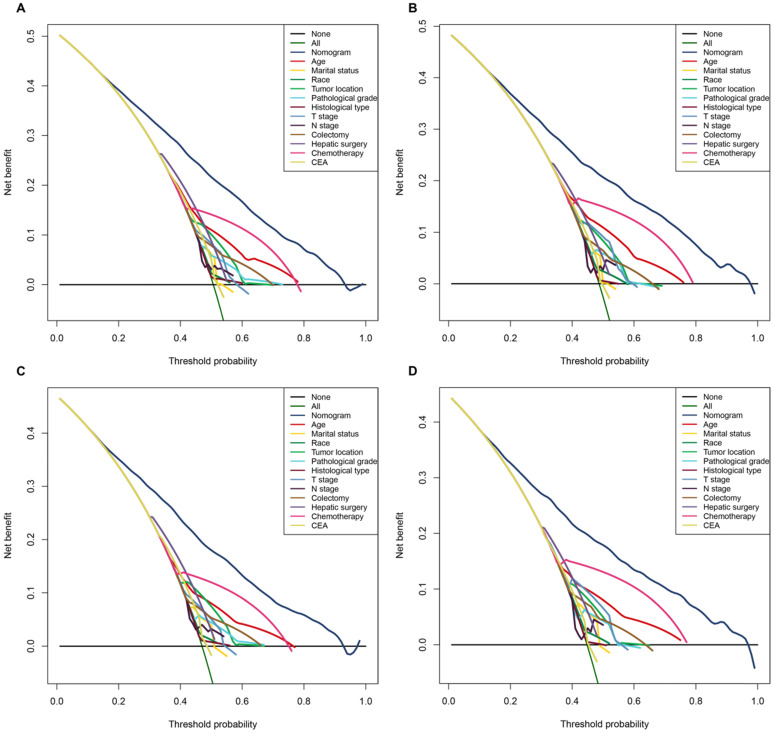
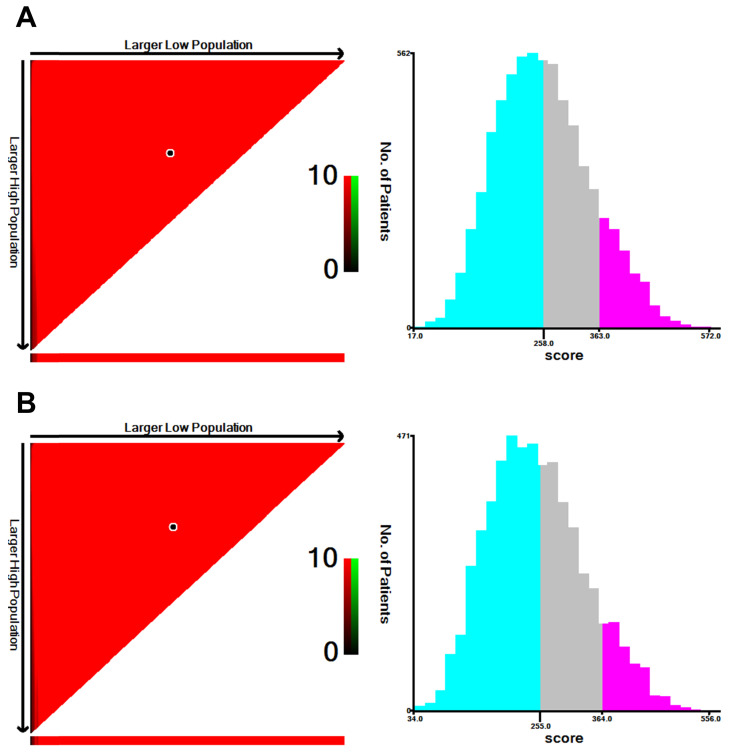
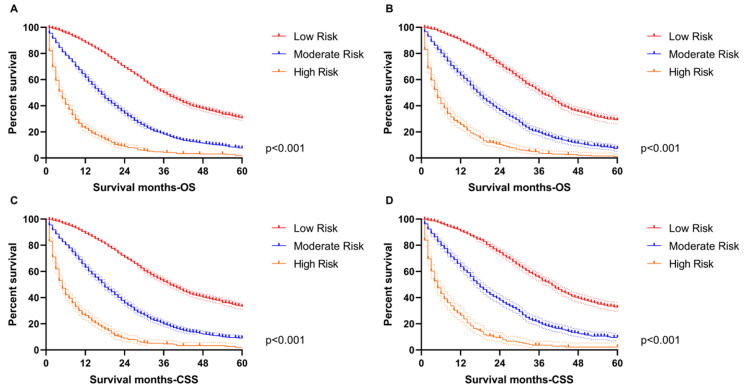
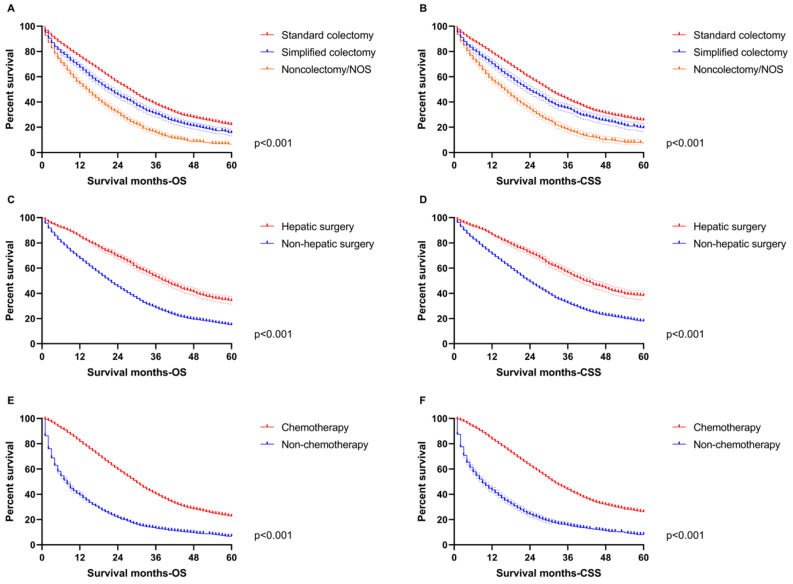
Background: Colorectal cancer (CRC) ranks as the third most frequent cancer type and the second leading cause of cancer-related death worldwide. The liver is the most common metastatic site of CRC with 20%-34% of patients suffering synchronous liver metastasis. Patients with colorectal liver-limited metastasis account for one-third of deaths from colorectal cancer. Moreover, some evidence indicated that CRC patients with synchronous liver disease encounter a worse prognosis and more disseminated disease state comparing with metastatic liver disease that develops metachronously. Methods: Data in this retrospective analysis were extracted from the Surveillance, Epidemiology, and End Results (SEER) database. Nomograms were constructed with basis from a multivariate Cox regression analysis. The prognostic nomograms were validated by C-index, time-dependent receiver operating characteristic (ROC) curve, decision curve analysis (DCA) and calibration curves. Results: A total of 9,958 CRC patients with synchronous liver-limited metastasis were extracted from the SEER database during 2010-2016. Both overall survival (OS) and cancer-specific survival (CSS) were significantly correlated with age, marital status, race, tumor location, pathological grade, histologic type, T stage, N stage, surgery for primary tumor, surgery for liver metastasis, chemotherapy and CEA. All of the significant variables were used to create the nomograms predicting OS and CSS. C-index values, time-dependent ROC curves, DCA curves and calibration curves, proved the superiority of the nomograms. Conclusions: Our research investigated a national cohort of almost 10,000 patients to create and verify nomograms based on pathological, therapeutic and demographic features to predict OS and CSS for synchronous colorectal liver-limited metastasis (SCLLM). The nomograms may act as an excellent tool to integrate clinical characteristics to guide the therapeutic choice for SCLLM patients.
Keywords: Nomogram; cancer-specific survival; colorectal cancer; liver metastasis; overall survival.
© The author(s).
Conflict of interest statement
Competing Interests: The authors have declared that no competing interest exists.
Figures
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2018;68:394–424. - PubMed
-
- Muratore A, Zorzi D, Bouzari H, Amisano M, Massucco P, Sperti E. et al. Asymptomatic colorectal cancer with un-resectable liver metastases: immediate colorectal resection or up-front systemic chemotherapy? Annals of surgical oncology. 2007;14:766–70. - PubMed
-
- Foster JH. Treatment of metastatic disease of the liver: a skeptic's view. Seminars in liver disease. 1984;4:170–9. - PubMed
-
- Kemeny N. Management of liver metastases from colorectal cancer. Oncology (Williston Park, NY) 2006;20:1161–76. 79; discussion 79-80, 85-6. - PubMed
LinkOut - more resources
Full Text Sources
