

Multiple flow-related intracranial aneurysms in the setting of contralateral carotid occlusion: Coincidence or association?
- PMID: 33033778
- PMCID: PMC7511913
- DOI: 10.4103/bc.bc_1_20
Multiple flow-related intracranial aneurysms in the setting of contralateral carotid occlusion: Coincidence or association?
Abstract
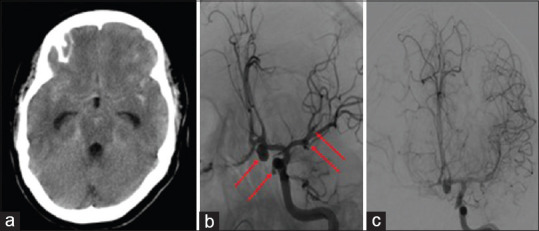
The prevalence of intracranial aneurysms (IAs) is higher in patients with internal carotid artery (ICA) stenosis, likely due to alterations in intracranial hemodynamics. Severe stenosis or occlusion of one ICA may result in increased demand and altered hemodynamics in the contralateral ICA, thus increasing the risk of contralateral IA formation. In this article, we discuss a relevant case and a comprehensive literature review as it pertains to the association of ICA stenosis and IA. Our patient was a 50-year-old female with a chronic asymptomatic right ICA occlusion who presented with diffuse subarachnoid hemorrhage. Emergent angiography revealed left-sided A1-A2 junction, paraclinoid, left middle cerebral artery (MCA) bifurcation, and left anterior temporal artery aneurysms. Brisk filling of the right anterior circulation through the anterior communicating artery was also identified, signifying increased demand on the left ICA circulation. Complete obliteration of all aneurysms was achieved with coil embolization and clipping. For our literature review, we searched the PubMed and EMBASE databases for case reports and case series, as well as references in previously published review articles that described patients with concurrent aneurysms and ICA stenosis. We selected articles that provided adequate information about the case presentations to compare aneurysm and patient characteristics. Our review revealed a higher number of patients with multiple aneurysms contralateral (25%) to rather than ipsilateral to (6%), the ICA stenosis. We discuss the pathogenesis and management of multiple flow-related IA in the context of the existing literature related to concurrent ICA stenosis and IA.
Keywords: Carotid stenosis; endovascular; flow-related aneurysm; intracranial aneurysm; neurosurgery; subarachnoid hemorrhage.
Copyright: © 2020 Brain Circulation.
Conflict of interest statement
There are no conflicts of interest.
Figures



Similar articles
-
[Arterial stenosis after coil migration in embolization of an aneurysm].No Shinkei Geka. 2010 Jan;38(1):41-5. No Shinkei Geka. 2010. PMID: 20085101 Japanese.
-
Spontaneous Thrombosis of a Giant Cavernous Internal Carotid Artery Aneurysm and Parent Vessel Occlusion in a Patient With Bilateral Cavernous Internal Carotid Artery Aneurysms.Cureus. 2023 Feb 20;15(2):e35231. doi: 10.7759/cureus.35231. eCollection 2023 Feb. Cureus. 2023. PMID: 36968945 Free PMC article.
-
Vertebral artery-to-middle cerebral artery bypass with coil embolization of giant internal carotid artery aneurysm: technical case report.Neurosurgery. 2005 May;56(5):E1159; discussion E1159. Neurosurgery. 2005. PMID: 15854269
-
Endovascular Management of Multiple Dysplastic Aneurysms in a Young Man with an Unknown Underlying Cause: A Case Report and Review of the Literature.World Neurosurg. 2018 Mar;111:349-357. doi: 10.1016/j.wneu.2017.12.129. Epub 2017 Dec 28. World Neurosurg. 2018. PMID: 29289804 Review.
-
Incidental intracranial aneurysms in patients with internal carotid artery stenosis: a CT angiography study and a metaanalysis.Stroke. 2009 Apr;40(4):1341-6. doi: 10.1161/STROKEAHA.108.538058. Epub 2009 Feb 19. Stroke. 2009. PMID: 19228836
Cited by
-
Multiple aneurysms coexisting with carotid occlusion revealed by cerebral infarction: A case report.Radiol Case Rep. 2022 Aug 29;17(11):4120-4122. doi: 10.1016/j.radcr.2022.07.116. eCollection 2022 Nov. Radiol Case Rep. 2022. PMID: 36072962 Free PMC article.
-
Structural Remodeling of the Extracellular Matrix in Arteriogenesis: A Review.Front Cardiovasc Med. 2021 Nov 5;8:761007. doi: 10.3389/fcvm.2021.761007. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34805316 Free PMC article. Review.
References
-
- Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011;10:626–36. - PubMed
-
- Bederson JB, Awad IA, Wiebers DO, Piepgras D, Haley EC, Jr, Brott T, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the Stroke Council of the American Heart Association. Stroke. 2011;31:2742–50. - PubMed
-
- Johnston SC, Selvin S, Gress DR. The burden, trends, and demographics of mortality from subarachnoid hemorrhage. Neurology. 1998;50:1413–8. - PubMed
-
- Lin N, Cahill KS, Frerichs KU, Friedlander RM, Claus EB. Treatment of ruptured and unruptured cerebral aneurysms in the USA: A paradigm shift. J Neurointerv Surg. 2018;10:i69–i76. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous