

Chest X-ray for predicting mortality and the need for ventilatory support in COVID-19 patients presenting to the emergency department
- PMID: 33033861
- PMCID: PMC7543667
- DOI: 10.1007/s00330-020-07270-1
Chest X-ray for predicting mortality and the need for ventilatory support in COVID-19 patients presenting to the emergency department
Abstract
Objectives: To evaluate the inter-rater agreement of chest X-ray (CXR) findings in coronavirus disease 2019 (COVID-19) and to determine the value of initial CXR along with demographic, clinical, and laboratory data at emergency department (ED) presentation for predicting mortality and the need for ventilatory support.
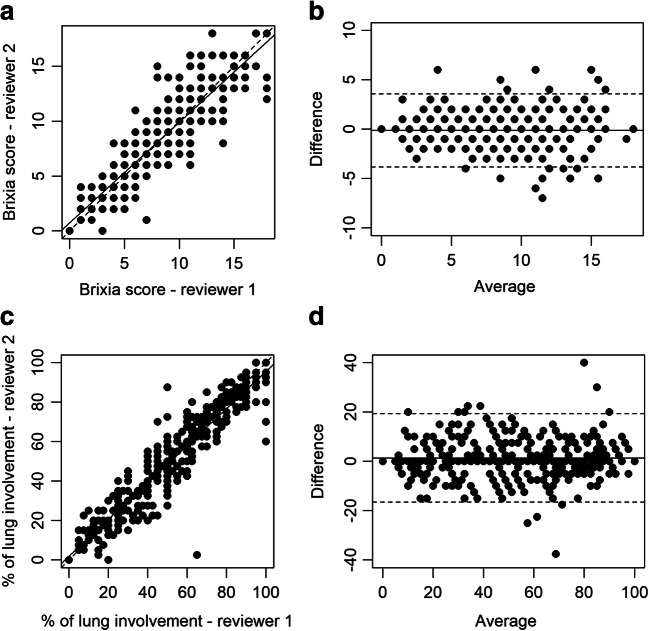
Methods: A total of 340 COVID-19 patients who underwent CXR in the ED setting (March 1-13, 2020) were retrospectively included. Two reviewers independently assessed CXR abnormalities, including ground-glass opacities (GGOs) and consolidation. Two scoring systems (Brixia score and percentage of lung involvement) were applied. Inter-rater agreement was assessed by weighted Cohen's kappa (κ) or intraclass correlation coefficient (ICC). Predictors of death and respiratory support were identified by logistic or Poisson regression.
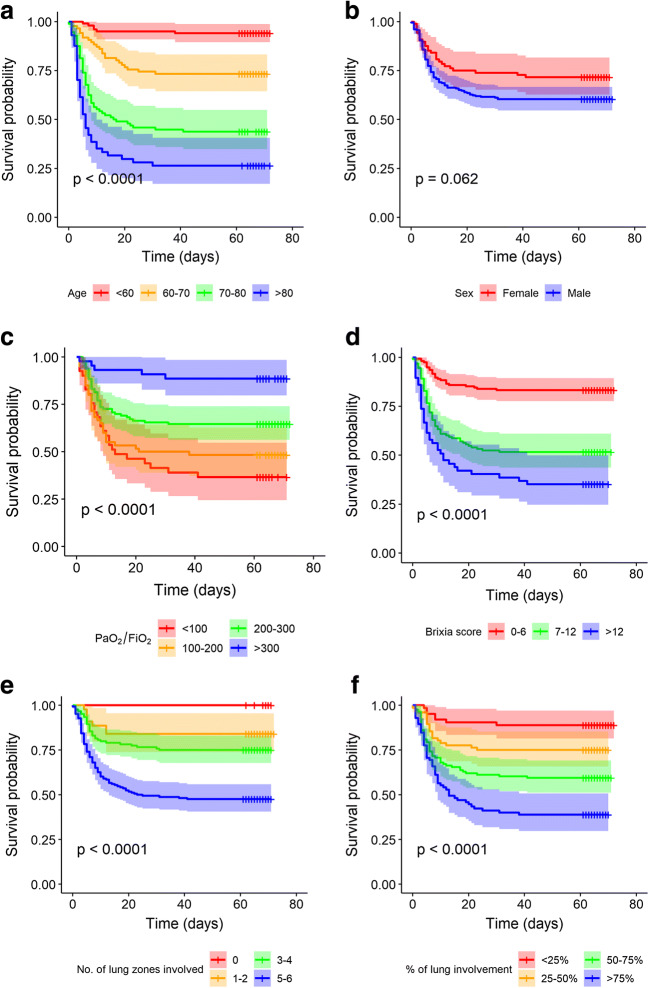
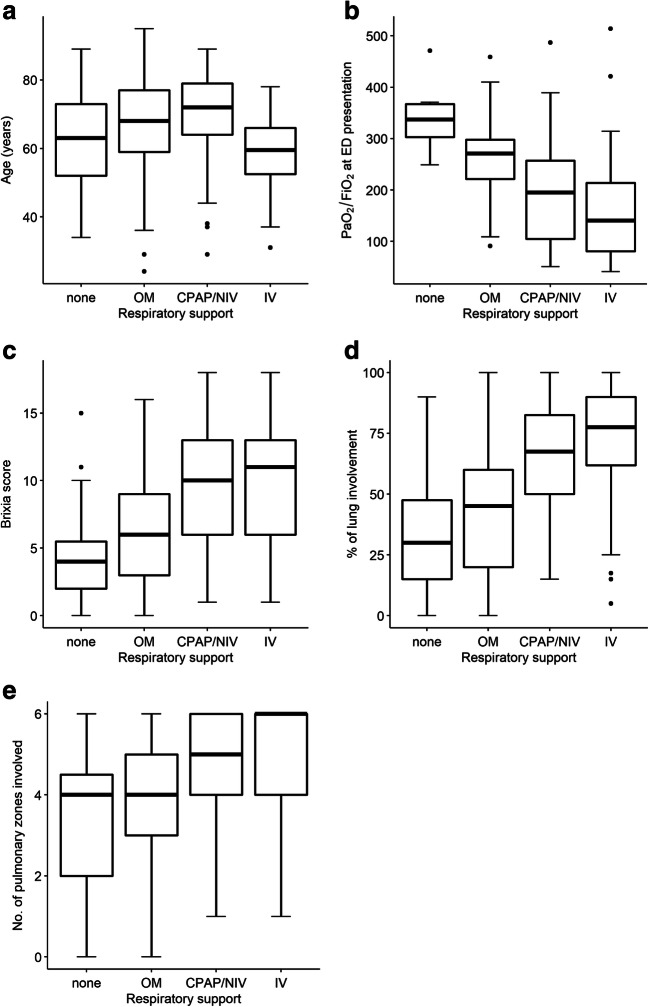
Results: GGO admixed with consolidation (n = 235, 69%) was the most common CXR finding. The inter-rater agreement was almost perfect for type of parenchymal opacity (κ = 0.90), Brixia score (ICC = 0.91), and percentage of lung involvement (ICC = 0.95). The Brixia score (OR: 1.19; 95% CI: 1.06, 1.34; p = 0.003), age (OR: 1.16; 95% CI: 1.11, 1.22; p < 0.001), PaO2/FiO2 ratio (OR: 0.99; 95% CI: 0.98, 1; p = 0.002), and cardiovascular diseases (OR: 3.21; 95% CI: 1.28, 8.39; p = 0.014) predicted death. Percentage of lung involvement (OR: 1.02; 95% CI: 1.01, 1.03; p = 0.001) and PaO2/FiO2 ratio (OR: 0.99; 95% CI: 0.99, 1.00; p < 0.001) were significant predictors of the need for ventilatory support.
Conclusions: CXR is a reproducible tool for assessing COVID-19 and integrates with patient history, PaO2/FiO2 ratio, and SpO2 values to early predict mortality and the need for ventilatory support.
Key points: • Chest X-ray is a reproducible tool for assessing COVID-19 pneumonia. • The Brixia score and percentage of lung involvement on chest X-ray integrate with patient history, PaO2/FIO2 ratio, and SpO2 values to early predict mortality and the need for ventilatory support in COVID-19 patients presenting to the emergency department.
Keywords: COVID-19; Radiography; Severe acute respiratory syndrome coronavirus 2.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures

References
-
- World Health Organization (2020) Clinical management of COVID-19: interim guidance, 27 May 2020 (No. WHO/2019-nCoV/clinical/2020.5). World Health Organization
