

Clinical Outcomes and Predictors in Patients With Unresectable Colorectal Cancer Liver Metastases Following Salvage Percutaneous Radiofrequency Ablation: A Single Center Preliminary Experience
- PMID: 33034276
- PMCID: PMC7549072
- DOI: 10.1177/1533033820963662
Clinical Outcomes and Predictors in Patients With Unresectable Colorectal Cancer Liver Metastases Following Salvage Percutaneous Radiofrequency Ablation: A Single Center Preliminary Experience
Abstract
Purpose: The purpose of this study was to investigate the clinical efficacy of salvage percutaneous radiofrequency ablation in patients with unresectable colorectal cancer liver metastases.
Methods: The cohort consisted of 81 patients with 126 colorectal cancer liver metastases who underwent radiofrequency ablation between January 2012 and September 2016. The clinical data and ablation data were retrospectively analyzed. The local tumor progression-free survival, overall survival, and prognostic factors were analyzed using the log-rank test and Cox regression model.
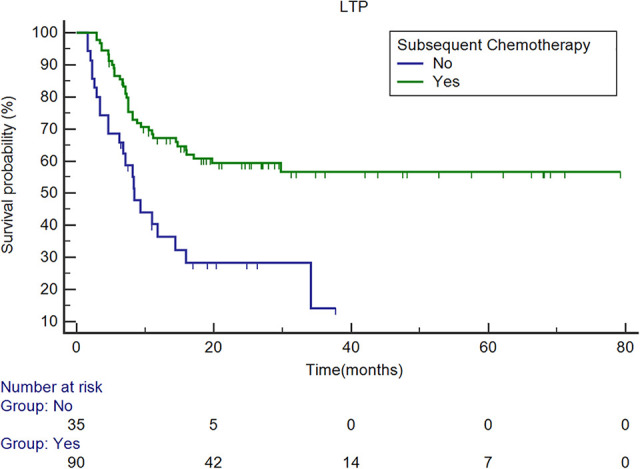
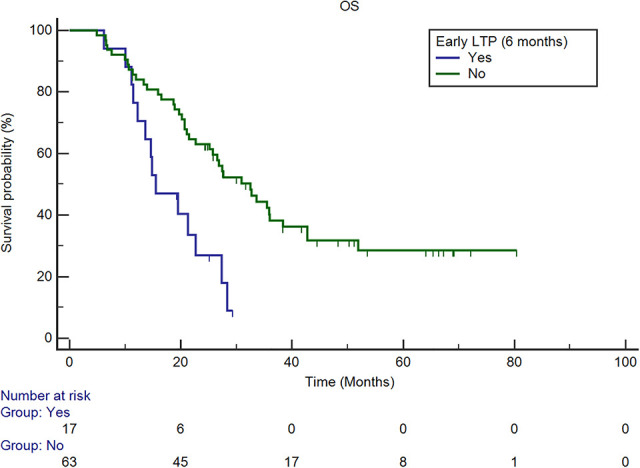
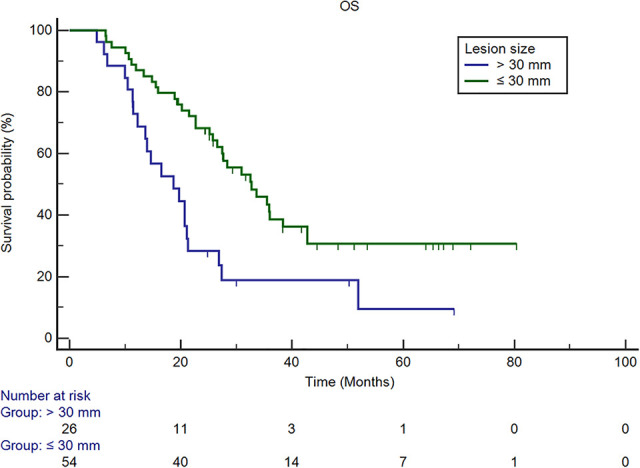
Results: The technique success rate was 99.21%. The primary efficacy rate was 100% at the 1-month follow-up. Minor complications were observed in 2 patients, which recovered within 1 week. The median local tumor progression-free survival time of all patients was 29.8 months. The absence of subsequent chemotherapy was an independent predictor of a shorter local tumor progression-free survival time (P < 0.001, hazard ratio: 2.823, 95% confidence interval: 1.603, 4.972). The median overall survival time was 26.8 months. A lesion size greater than 3 cm (P = 0.011, hazard ratio: 2.112, 95% confidence interval: 1.188, 3.754) and the presence of early local tumor progression (P = 0.011, hazard ratio: 2.352, 95% confidence interval: 1.217, 4.545) were related to a shorter survival time.
Conclusions: Percutaneous radiofrequency ablation is safe in patients with colorectal cancer liver metastases refractory from chemotherapy. Subsequent chemotherapy is important to enhance local control. Small lesions and favorable early responses are related to prolonged overall survival.
Keywords: colorectal cancer liver metastases; local tumor progression; overall survival; predictor; radiofrequency ablation; unresectable.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442 - PubMed
-
- Leonard GD, Brenner B, Kemeny NE. Neoadjuvant chemotherapy before liver resection for patients with unresectable liver metastases from colorectal carcinoma. J Clin Oncol. 2005;23(9):2038–2048. doi:10.1200/JCO.2005.00.349 - PubMed
-
- Folprecht G, Gruenberger T, Bechstein WO, et al. Tumour response and secondary resectability of colorectal liver metastases following neoadjuvant chemotherapy with cetuximab: the CELIM randomised phase 2 trial. Lancet Oncol. 2010;11(1):38–47. doi:10.1016/S1470-2045(09)70330-4 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
