

Time-varying age- and CD4-stratified rates of mortality and WHO stage 3 and stage 4 events in children, adolescents and youth 0 to 24 years living with perinatally acquired HIV, before and after antiretroviral therapy initiation in the paediatric IeDEA Global Cohort Consortium
- PMID: 33034417
- PMCID: PMC7545918
- DOI: 10.1002/jia2.25617
Time-varying age- and CD4-stratified rates of mortality and WHO stage 3 and stage 4 events in children, adolescents and youth 0 to 24 years living with perinatally acquired HIV, before and after antiretroviral therapy initiation in the paediatric IeDEA Global Cohort Consortium
Abstract
Introduction: Evaluating outcomes of paediatric patients with HIV provides crucial data for clinicians and policymakers. We analysed mortality and clinical events rates among children, adolescents, and youth with perinatally acquired HIV (PHIV) aged 0 to 24 years stratified by time-varying age and CD4, before and after antiretroviral therapy (ART), in the paediatric IeDEA multiregional collaboration (East, West, Central and Southern Africa, Asia-Pacific, and Central/South America and the Caribbean).
Methods: ART-naïve children with HIV enrolled before age 10 (proxy for perinatal infection) at IeDEA sites between 2004 and 2016, with ≥1 CD4 measurement during follow-up were included. We estimated incidence rates (IR) and 95% confidence intervals (95% CI) of mortality and first occurrence of WHO-4 and WHO-3 events, excluding tuberculosis, during person-years (PY) spent within different age (<2, 2 to 4, 5 to 9, 10 to 14, 15 to 19, 20 to 24) and CD4 (percent when <5 years [<15%, 15% to 24%, ≥25%]; count when ≥5 years [<200, 200 to 499, ≥500 cells/µL]) strata. We used linear mixed models to predict CD4 evolution, with trends modelled by region.
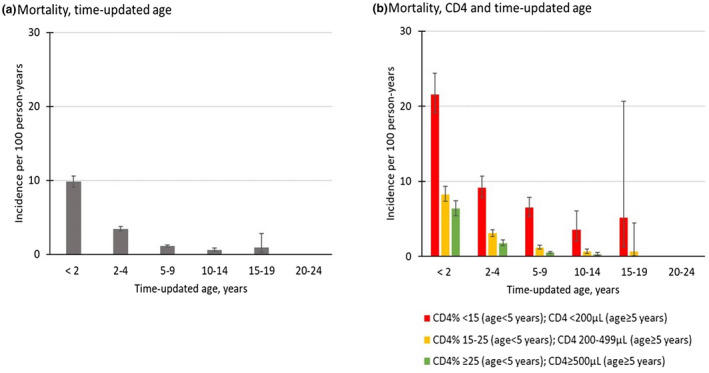
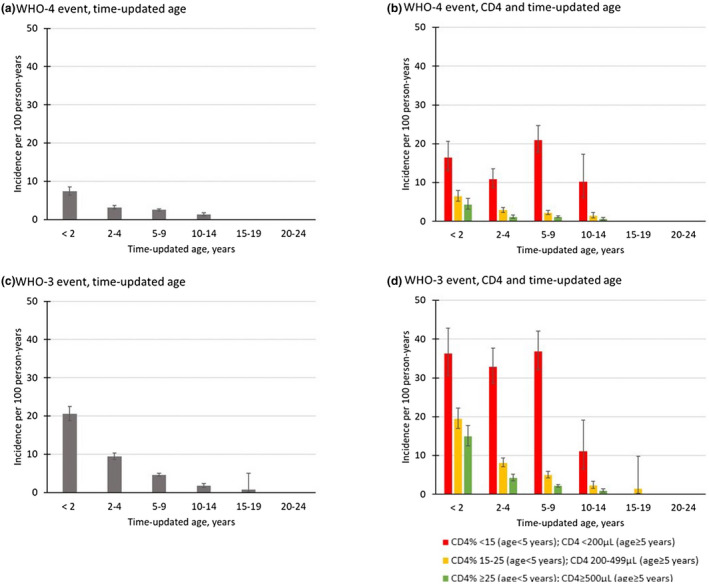
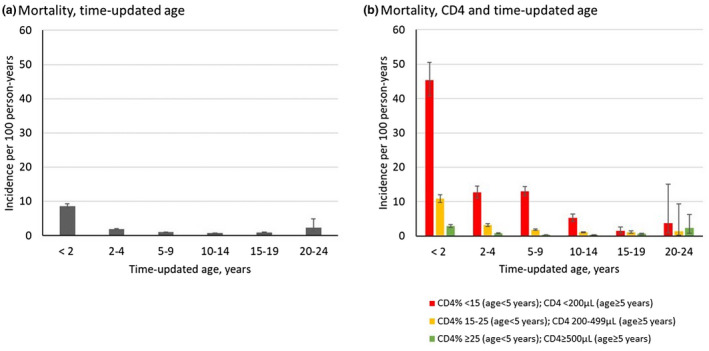
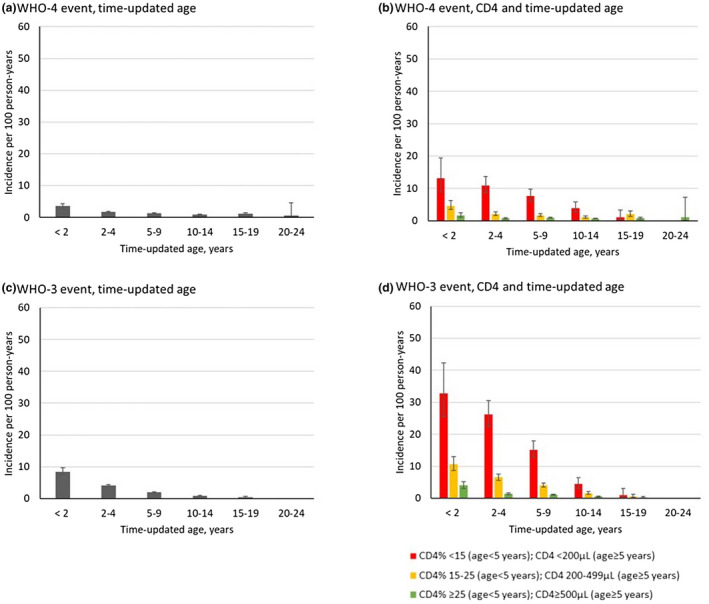
Results: In the pre-ART period, 49 137 participants contributed 51 966 PY of follow-up (median enrolment age: 3.9 years). The overall pre-ART IRs were 2.8/100 PY (95% CI: 2.7 to 2.9) for mortality, 3.3/100 PY (95% CI: 3.0 to 3.5) for first occurrence of a WHO-4 event, and 7.0/100 PY (95% CI: 6.7 to 7.4) for first occurrence of a WHO-3 event. Lower CD4 and younger age strata were associated with increased rates of both mortality and first occurrence of a clinical event. In the post-ART period, 52 147 PHIVY contributed 207 945 PY (ART initiation median age: 4.5 years). Overall mortality IR was 1.4/100 PY (95% CI: 1.4 to 1.5) and higher in low CD4 strata; patients at each end of the age spectrum (<2 and >19) had increased mortality post-ART. IRs for first occurrence of WHO-4 and WHO-3 events were 1.3/100 PY (95% CI: 1.2 to 1.4) and 2.1/100 PY (95% CI: 2.0 to 2.2) respectively. These were also associated with lower CD4 and younger age strata.
Conclusions: Mortality and incidence of clinical events were highest in both younger (<2 years) and older (>19 years) youth with PHIV. Scaling-up services for <2 years (early access to HIV diagnosis and care) and >19 years (adolescent- and youth-focused health services) is critical to improve outcomes among PHIVY.
Keywords: HIV; adolescents; mortality; paediatrics; severe morbidity.
© 2020 The Authors. Journal of the International AIDS Society published by John Wiley & Sons Ltd on behalf of the International AIDS Society.
Figures
References
-
- Azcoaga‐Lorenzo A, Ferreyra C, Alvarez A, Palma P, Velilla E, Del Amo J. Effectiveness of a PMTCT programme in rural Western Kenya. AIDS Care. 2011;23(3):274–80. - PubMed
-
- World Health Organisation . UNAIDS Data 2018. 2018. Available from: http://www.unaids.org/sites/default/files/media_asset/unaids‐data‐2018_e...
-
- Johnson LF, Davies MA, Moultrie H, Sherman GG, Bland RM, Rehle TM, et al. The effect of early initiation of antiretroviral treatment in infants on pediatric AIDS mortality in South Africa: a model‐based analysis. Pediatr Infect Dis J. 2012;31(5):474–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL/NHLBI NIH HHS/United States
- U01 AI096299/AI/NIAID NIH HHS/United States
- K08 HD094638/NH/NIH HHS/United States
- AA/NIAAA NIH HHS/United States
- MH/NIMH NIH HHS/United States
- LM/NLM NIH HHS/United States
- U01AI069924/NH/NIH HHS/United States
- U01AI069907/NH/NIH HHS/United States
- R01 HD079214/HD/NICHD NIH HHS/United States
- U01 AI069911/AI/NIAID NIH HHS/United States
- CA/NCI NIH HHS/United States
- U01 AI069907/AI/NIAID NIH HHS/United States
- U01AI096299/NH/NIH HHS/United States
- TW/FIC NIH HHS/United States
- U01AI069923/NH/NIH HHS/United States
- U01AI069919/NH/NIH HHS/United States
- U01 AI069923/AI/NIAID NIH HHS/United States
- R24 AI124872/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- U01 AI069919/AI/NIAID NIH HHS/United States
- DK/NIDDK NIH HHS/United States
- R01HD079214/NH/NIH HHS/United States
- P30 AI060354/AI/NIAID NIH HHS/United States
- DA/NIDA NIH HHS/United States
- U01AI069911/NH/NIH HHS/United States
- K08 HD094638/HD/NICHD NIH HHS/United States
- U01 AI069924/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
