

Comparison of Chest Radiograph Interpretations by Artificial Intelligence Algorithm vs Radiology Residents
- PMID: 33034642
- PMCID: PMC7547369
- DOI: 10.1001/jamanetworkopen.2020.22779
Comparison of Chest Radiograph Interpretations by Artificial Intelligence Algorithm vs Radiology Residents
Abstract
Importance: Chest radiography is the most common diagnostic imaging examination performed in emergency departments (EDs). Augmenting clinicians with automated preliminary read assistants could help expedite their workflows, improve accuracy, and reduce the cost of care.
Objective: To assess the performance of artificial intelligence (AI) algorithms in realistic radiology workflows by performing an objective comparative evaluation of the preliminary reads of anteroposterior (AP) frontal chest radiographs performed by an AI algorithm and radiology residents.
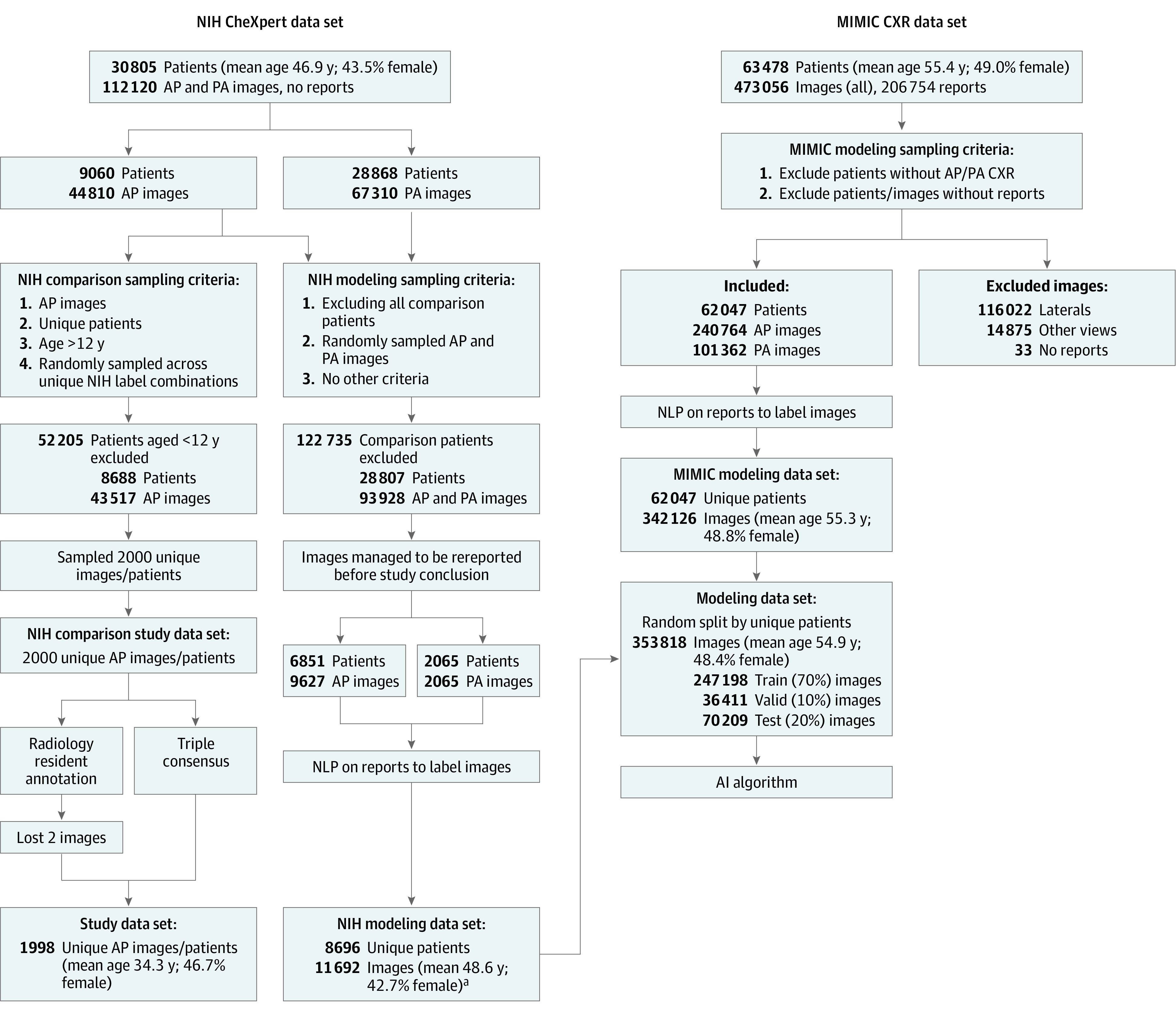
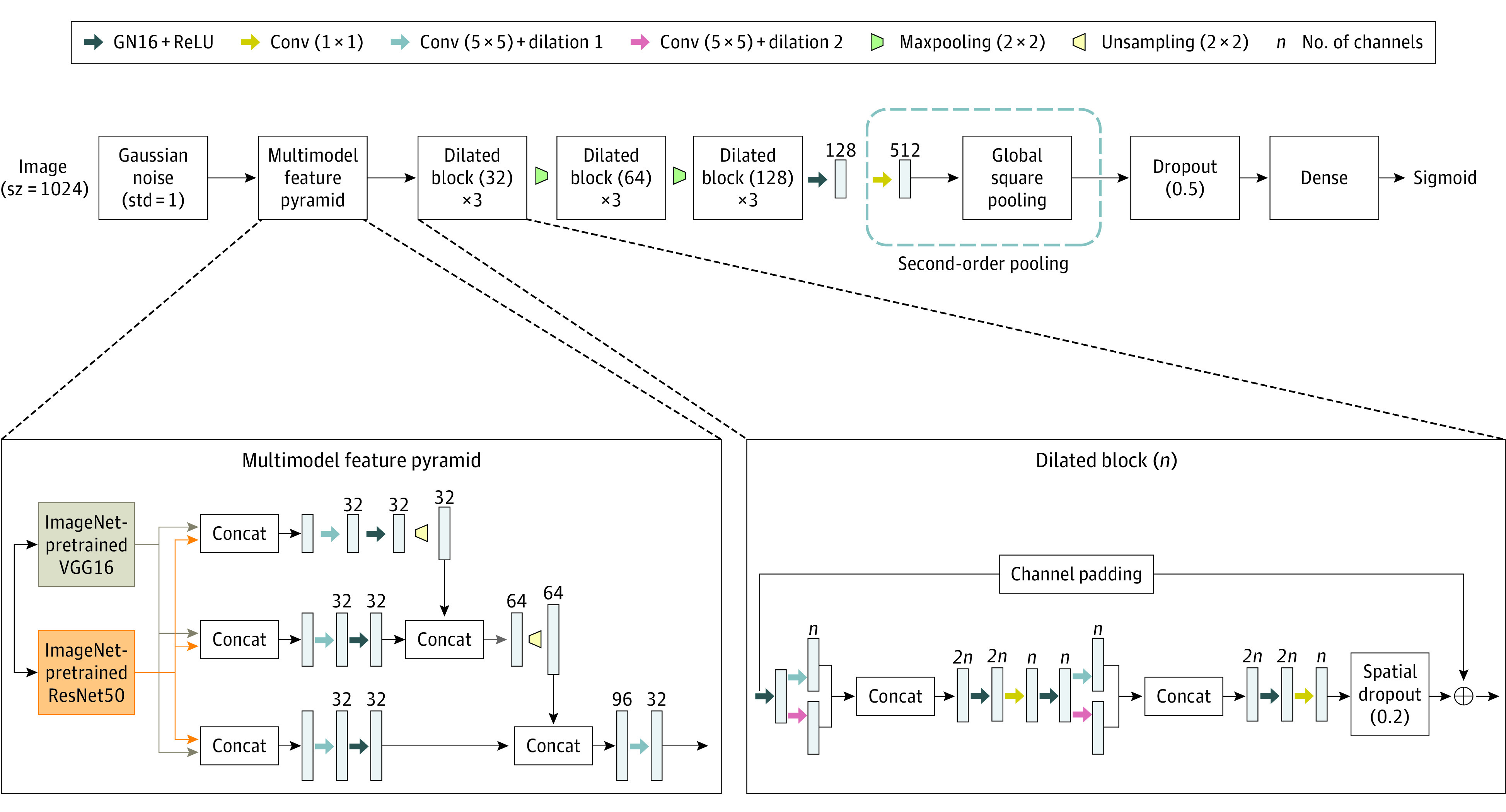
Design, setting, and participants: This diagnostic study included a set of 72 findings assembled by clinical experts to constitute a full-fledged preliminary read of AP frontal chest radiographs. A novel deep learning architecture was designed for an AI algorithm to estimate the findings per image. The AI algorithm was trained using a multihospital training data set of 342 126 frontal chest radiographs captured in ED and urgent care settings. The training data were labeled from their associated reports. Image-based F1 score was chosen to optimize the operating point on the receiver operating characteristics (ROC) curve so as to minimize the number of missed findings and overcalls per image read. The performance of the model was compared with that of 5 radiology residents recruited from multiple institutions in the US in an objective study in which a separate data set of 1998 AP frontal chest radiographs was drawn from a hospital source representative of realistic preliminary reads in inpatient and ED settings. A triple consensus with adjudication process was used to derive the ground truth labels for the study data set. The performance of AI algorithm and radiology residents was assessed by comparing their reads with ground truth findings. All studies were conducted through a web-based clinical study application system. The triple consensus data set was collected between February and October 2018. The comparison study was preformed between January and October 2019. Data were analyzed from October to February 2020. After the first round of reviews, further analysis of the data was performed from March to July 2020.
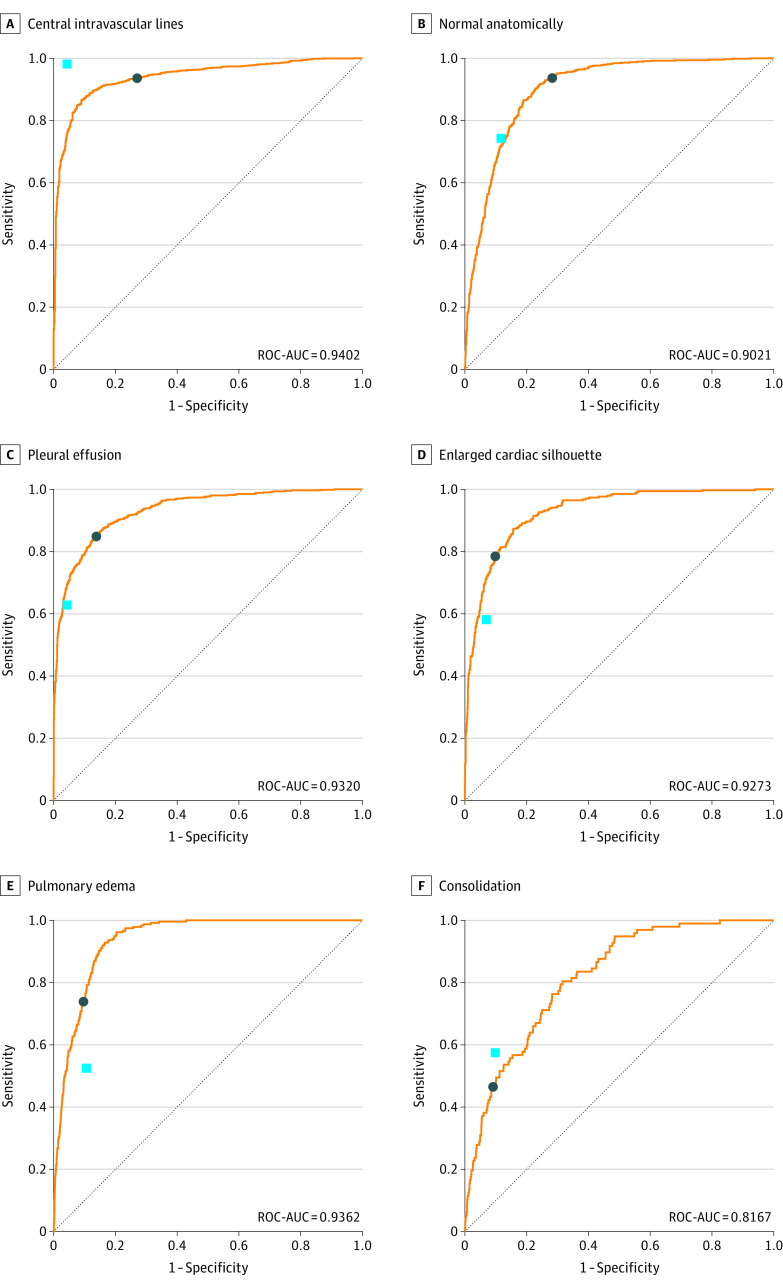
Main outcomes and measures: The learning performance of the AI algorithm was judged using the conventional ROC curve and the area under the curve (AUC) during training and field testing on the study data set. For the AI algorithm and radiology residents, the individual finding label performance was measured using the conventional measures of label-based sensitivity, specificity, and positive predictive value (PPV). In addition, the agreement with the ground truth on the assignment of findings to images was measured using the pooled κ statistic. The preliminary read performance was recorded for AI algorithm and radiology residents using new measures of mean image-based sensitivity, specificity, and PPV designed for recording the fraction of misses and overcalls on a per image basis. The 1-sided analysis of variance test was used to compare the means of each group (AI algorithm vs radiology residents) using the F distribution, and the null hypothesis was that the groups would have similar means.
Results: The trained AI algorithm achieved a mean AUC across labels of 0.807 (weighted mean AUC, 0.841) after training. On the study data set, which had a different prevalence distribution, the mean AUC achieved was 0.772 (weighted mean AUC, 0.865). The interrater agreement with ground truth finding labels for AI algorithm predictions had pooled κ value of 0.544, and the pooled κ for radiology residents was 0.585. For the preliminary read performance, the analysis of variance test was used to compare the distributions of AI algorithm and radiology residents' mean image-based sensitivity, PPV, and specificity. The mean image-based sensitivity for AI algorithm was 0.716 (95% CI, 0.704-0.729) and for radiology residents was 0.720 (95% CI, 0.709-0.732) (P = .66), while the PPV was 0.730 (95% CI, 0.718-0.742) for the AI algorithm and 0.682 (95% CI, 0.670-0.694) for the radiology residents (P < .001), and specificity was 0.980 (95% CI, 0.980-0.981) for the AI algorithm and 0.973 (95% CI, 0.971-0.974) for the radiology residents (P < .001).
Conclusions and relevance: These findings suggest that it is possible to build AI algorithms that reach and exceed the mean level of performance of third-year radiology residents for full-fledged preliminary read of AP frontal chest radiographs. This diagnostic study also found that while the more complex findings would still benefit from expert overreads, the performance of AI algorithms was associated with the amount of data available for training rather than the level of difficulty of interpretation of the finding. Integrating such AI systems in radiology workflows for preliminary interpretations has the potential to expedite existing radiology workflows and address resource scarcity while improving overall accuracy and reducing the cost of care.
Conflict of interest statement
Figures
Comment in
-
Artificial intelligence, chest radiographs, and radiology trainees: a powerful combination to enhance the future of radiologists?Quant Imaging Med Surg. 2021 May;11(5):2204-2207. doi: 10.21037/qims-20-1306. Quant Imaging Med Surg. 2021. PMID: 33937001 Free PMC article. No abstract available.
References
-
- Kane L. Medscape national physician burnout, depression and suicide report 2019. Medscape. January 16, 2019. Accessed September 11, 2020. https://www.medscape.com/slideshow/2019-lifestyle-burnout-depression-601...
-
- Wang X, Peng Y, Lu L, Lu Z, Bagheri M SR. ChestX-ray8: hospital-scale chest x-ray database and benchmarks on weakly-supervised classification and localization of common thorax diseases. Paper presented at: 2017 IEEE Conference on Computer Vision and Pattern Recognition; July 21-26, 2017; Honolulu, HI. Accessed September 11, 2020. doi: 10.1109/CVPR.2017.369 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
