

Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study
- PMID: 33034686
- PMCID: PMC7880913
- DOI: 10.1007/s00134-020-06234-9
Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study
Erratum in
-
Correction to: Prevalence, associated factors and outcomes of pressure injuries in adult intensive care unit patients: the DecubICUs study.Intensive Care Med. 2021 Apr;47(4):503-520. doi: 10.1007/s00134-020-06327-5. Intensive Care Med. 2021. PMID: 33635356 Free PMC article. No abstract available.
Abstract
Purpose: Intensive care unit (ICU) patients are particularly susceptible to developing pressure injuries. Epidemiologic data is however unavailable. We aimed to provide an international picture of the extent of pressure injuries and factors associated with ICU-acquired pressure injuries in adult ICU patients.
Methods: International 1-day point-prevalence study; follow-up for outcome assessment until hospital discharge (maximum 12 weeks). Factors associated with ICU-acquired pressure injury and hospital mortality were assessed by generalised linear mixed-effects regression analysis.
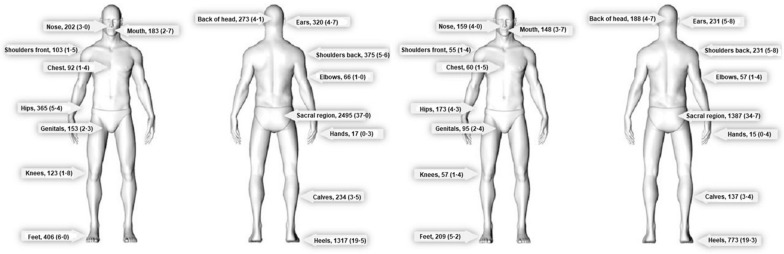
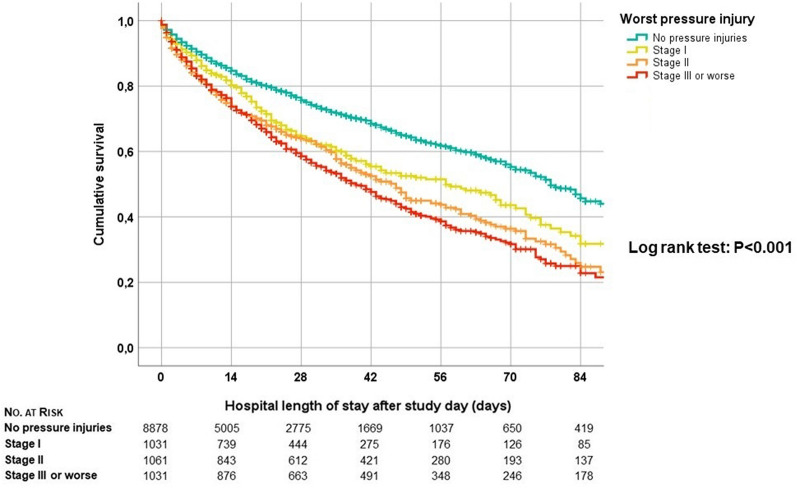
Results: Data from 13,254 patients in 1117 ICUs (90 countries) revealed 6747 pressure injuries; 3997 (59.2%) were ICU-acquired. Overall prevalence was 26.6% (95% confidence interval [CI] 25.9-27.3). ICU-acquired prevalence was 16.2% (95% CI 15.6-16.8). Sacrum (37%) and heels (19.5%) were most affected. Factors independently associated with ICU-acquired pressure injuries were older age, male sex, being underweight, emergency surgery, higher Simplified Acute Physiology Score II, Braden score < 19, ICU stay > 3 days, comorbidities (chronic obstructive pulmonary disease, immunodeficiency), organ support (renal replacement, mechanical ventilation on ICU admission), and being in a low or lower-middle income-economy. Gradually increasing associations with mortality were identified for increasing severity of pressure injury: stage I (odds ratio [OR] 1.5; 95% CI 1.2-1.8), stage II (OR 1.6; 95% CI 1.4-1.9), and stage III or worse (OR 2.8; 95% CI 2.3-3.3).
Conclusion: Pressure injuries are common in adult ICU patients. ICU-acquired pressure injuries are associated with mainly intrinsic factors and mortality. Optimal care standards, increased awareness, appropriate resource allocation, and further research into optimal prevention are pivotal to tackle this important patient safety threat.
Keywords: Decubitus epidemiology; ICU; Morbidity; Mortality; Outcome; Pressure injury; Pressure ulcer; Risk factors.
Conflict of interest statement
Received honoraria or grants outside the submitted work: Ashish K. Khanna (Medtronic, Philips North America, Edwards Lifesciences, Zoll Medical, La Jolla pharmaceuticals, and Retia Medical). Stijn I. Blot (Pfizer, 3M). Leif Saager (Medtronic, Merck, The 37 Company, Ferrer Deutschland). For the other authors, there are no conflicts of interest.
Figures
Comment in
-
Leaving a mark: pressure injury research in the intensive care unit.Intensive Care Med. 2021 Feb;47(2):222-224. doi: 10.1007/s00134-021-06350-0. Epub 2021 Jan 27. Intensive Care Med. 2021. PMID: 33502541 Free PMC article. No abstract available.
References
-
- National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific Pressure Injury Alliance . Prevention and treatment of pressure ulcers: Clinical practice guideline. Osborne Park: Cambridge Media; 2019.
-
- National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel, and Pan Pacific Pressure Injury Alliance . Prevention and treatment of pressure ulcers: clinical practice guideline. Osborne Park: Cambridge Media; 2014.
-
- National Pressure Ulcer Advisory Panel (2017) NPUAP position statement on staging—2017 clarifications. https://npuap.org/page/PositionStatements. Accessed 25 Aug 2019
-
- Gefen A (2008) How much time does it take to get a pressure ulcer? Integrated evidence from human, animal, and in vitro studies. Ostomy Wound Manag 54:26–28, 30-25 - PubMed
