

Fine Particulate Matter Exposure and Cancer Incidence: Analysis of SEER Cancer Registry Data from 1992-2016
- PMID: 33035119
- PMCID: PMC7546438
- DOI: 10.1289/EHP7246
Fine Particulate Matter Exposure and Cancer Incidence: Analysis of SEER Cancer Registry Data from 1992-2016
Abstract
Background: Previous research has identified an association between fine particulate matter () air pollution and lung cancer. Most of the evidence for this association, however, is based on research using lung cancer mortality, not incidence. Research that examines potential associations between and incidence of non-lung cancers is limited.
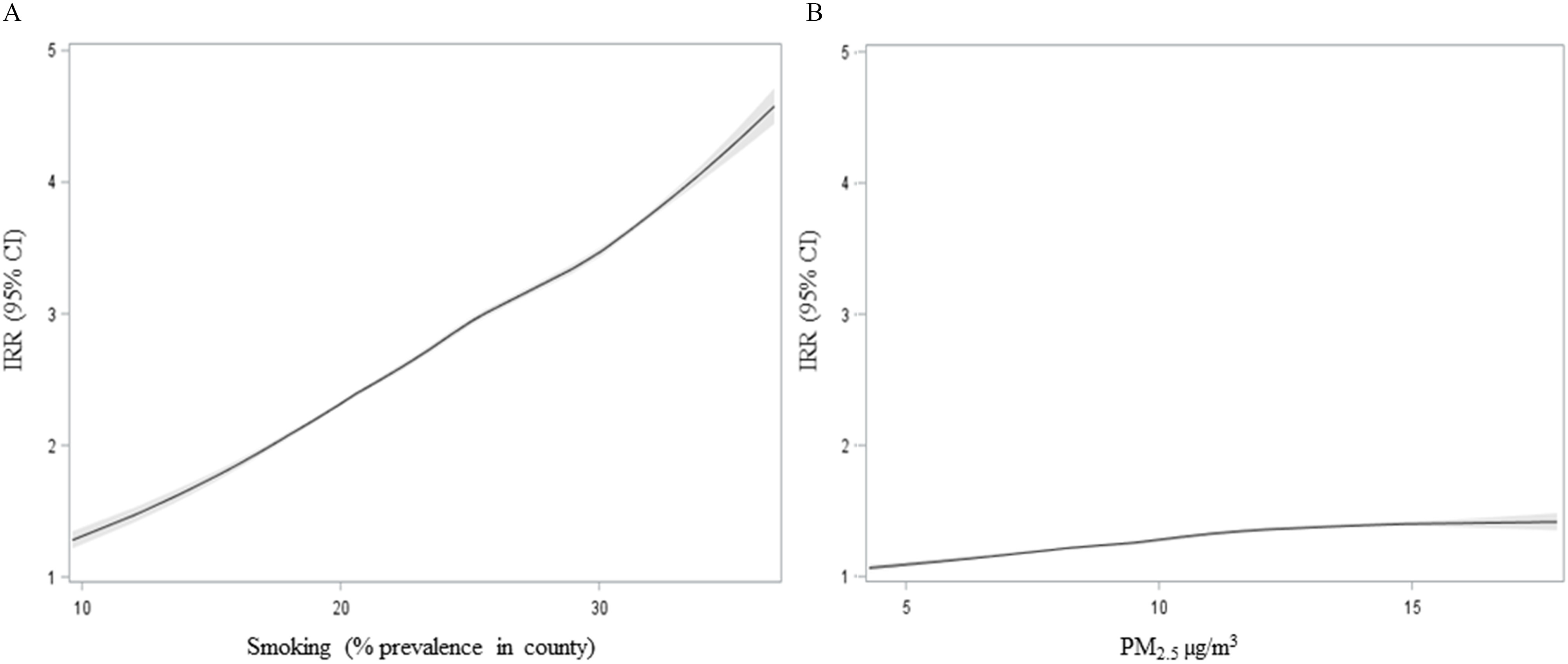
Objectives: The primary purpose of this study was to evaluate the association between the incidence of cancer and exposure to using cases of cancer incidences from U.S. registries. Secondary objectives include evaluating the sensitivity of the associations to model selection, spatial control, and latency period as well as estimating the exposure-response relationship for several cancer types.
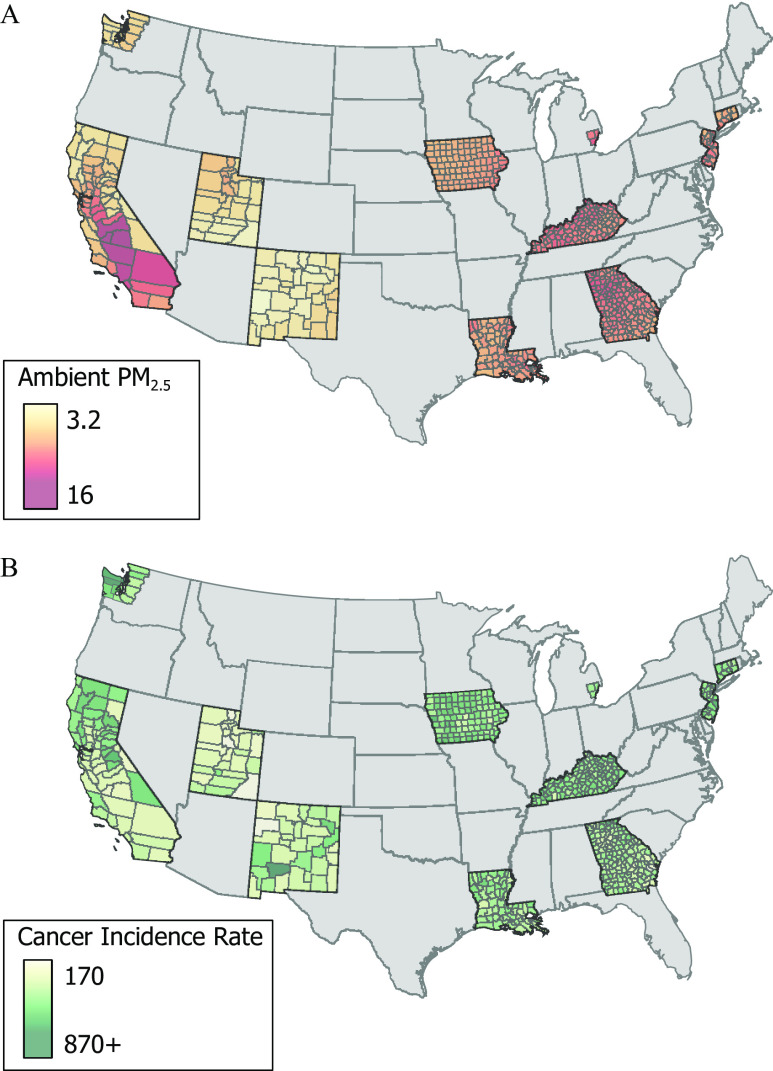
Methods: Surveillance, Epidemiology, and End Results (SEER) program data were used to calculate incidence rates for various cancer types in 607 U.S. counties. County-level concentrations were estimated using integrated empirical geographic regression models. Flexible semi-nonparametric regression models were used to estimate associations between and cancer incidence for selected cancers while controlling for important county-level covariates. Primary time-independent models using average incidence rates from 1992-2016 and average from 1988-2015 were estimated. In addition, time-varying models using annual incidence rates from 2002-2011 and lagged moving averages of annual estimates for were also estimated.
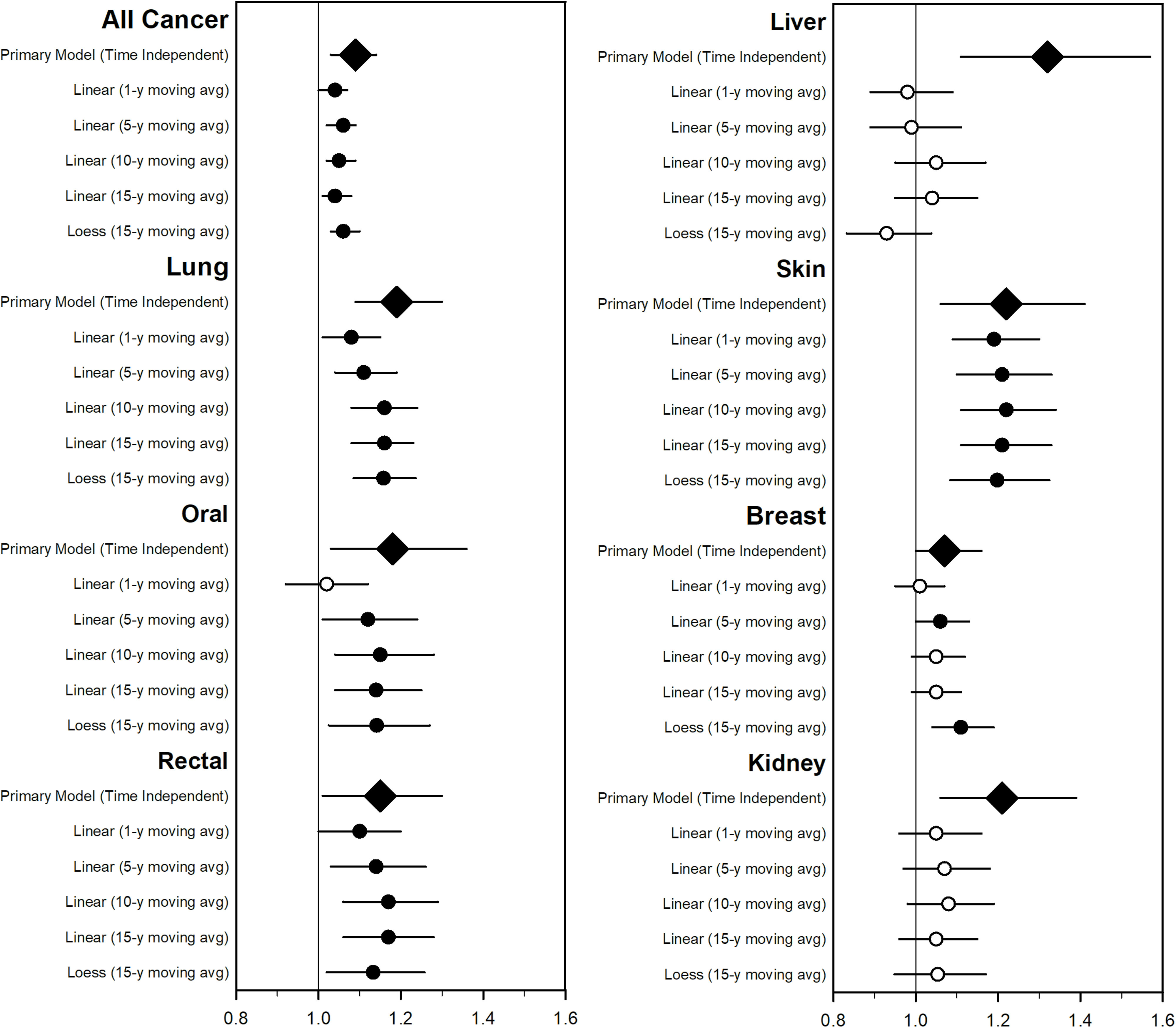
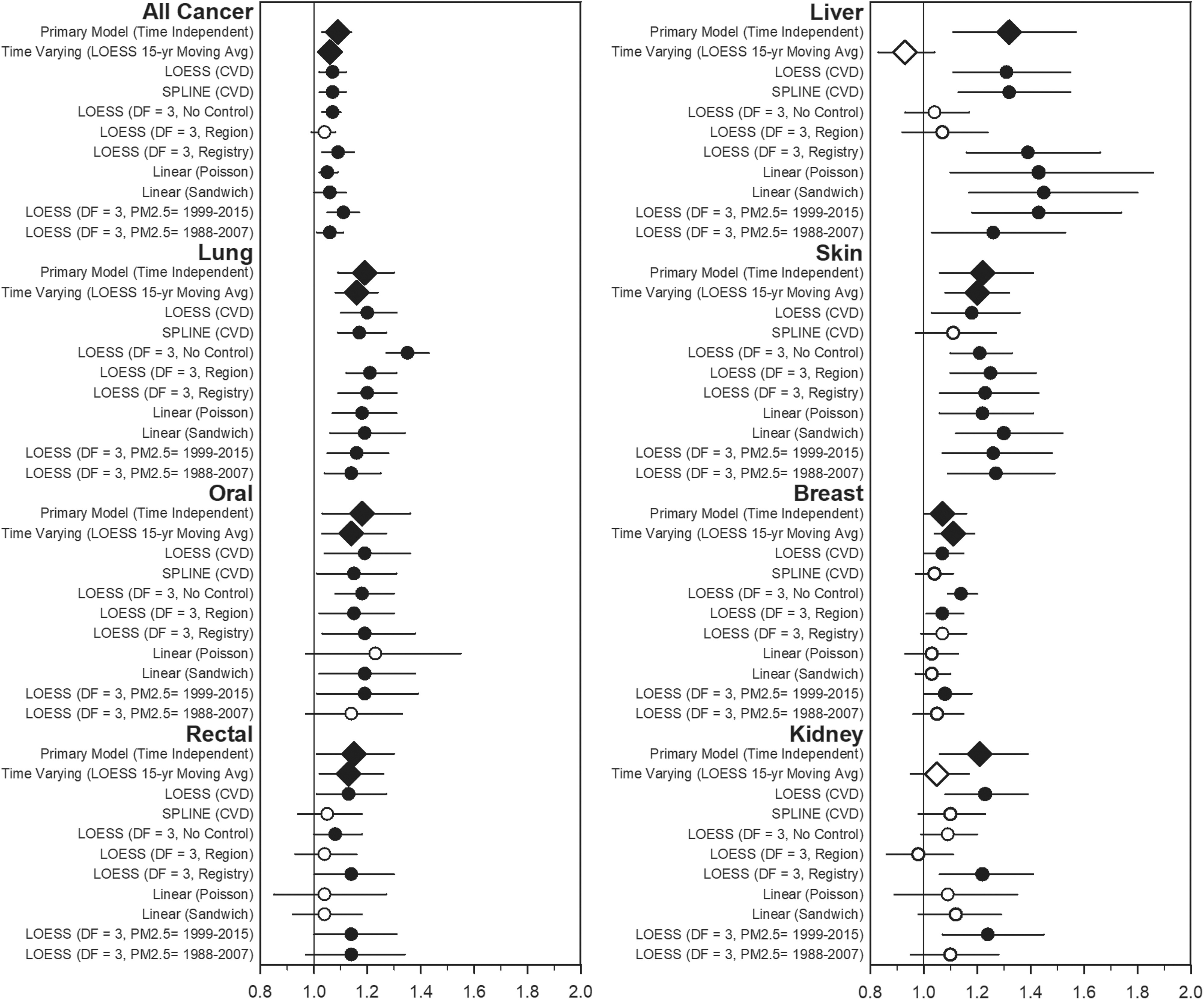
Results: The incidences of all cancer and lung cancer were consistently associated with . The incident rate ratios (IRRs), per increase in , for all and lung cancer were 1.09 (95% CI: 1.03, 1.14) and 1.19 (95% CI: 1.09, 1.30), respectively. Less robust associations were observed with oral, rectal, liver, skin, breast, and kidney cancers.
Discussion: Exposure to air pollution contributes to lung cancer incidence and is potentially associated with non-lung cancer incidence. https://doi.org/10.1289/EHP7246.
Figures
References
-
- Ancona C, Badaloni C, Mataloni F, Bolignano A, Bucci S, Cesaroni G, et al. . 2015. Mortality and morbidity in a population exposed to multiple sources of air pollution: a retrospective cohort study using air dispersion models. Environ Res 137:467–474, PMID: 25701728, 10.1016/j.envres.2014.10.036. - DOI - PubMed
-
- Bai L, Shin S, Burnett RT, Kwong JC, Hystad P, van Donkelaar A, et al. . 2020. Exposure to ambient air pollution and the incidence of lung cancer and breast cancer in the Ontario Population Health and Environment Cohort. Int J Cancer 146(9):2450–2459, PMID: 31304979, 10.1002/ijc.32575. - DOI - PubMed
-
- Benjamini Y, Hochberg Y. 1995. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Series B Stat Methodol 57(1):289–300, 10.1111/j.2517-6161.1995.tb02031.x. - DOI
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
