

Immunotherapy efficacy on mismatch repair-deficient colorectal cancer: From bench to bedside
- PMID: 33035640
- PMCID: PMC7886024
- DOI: 10.1016/j.bbcan.2020.188447
Immunotherapy efficacy on mismatch repair-deficient colorectal cancer: From bench to bedside
Abstract
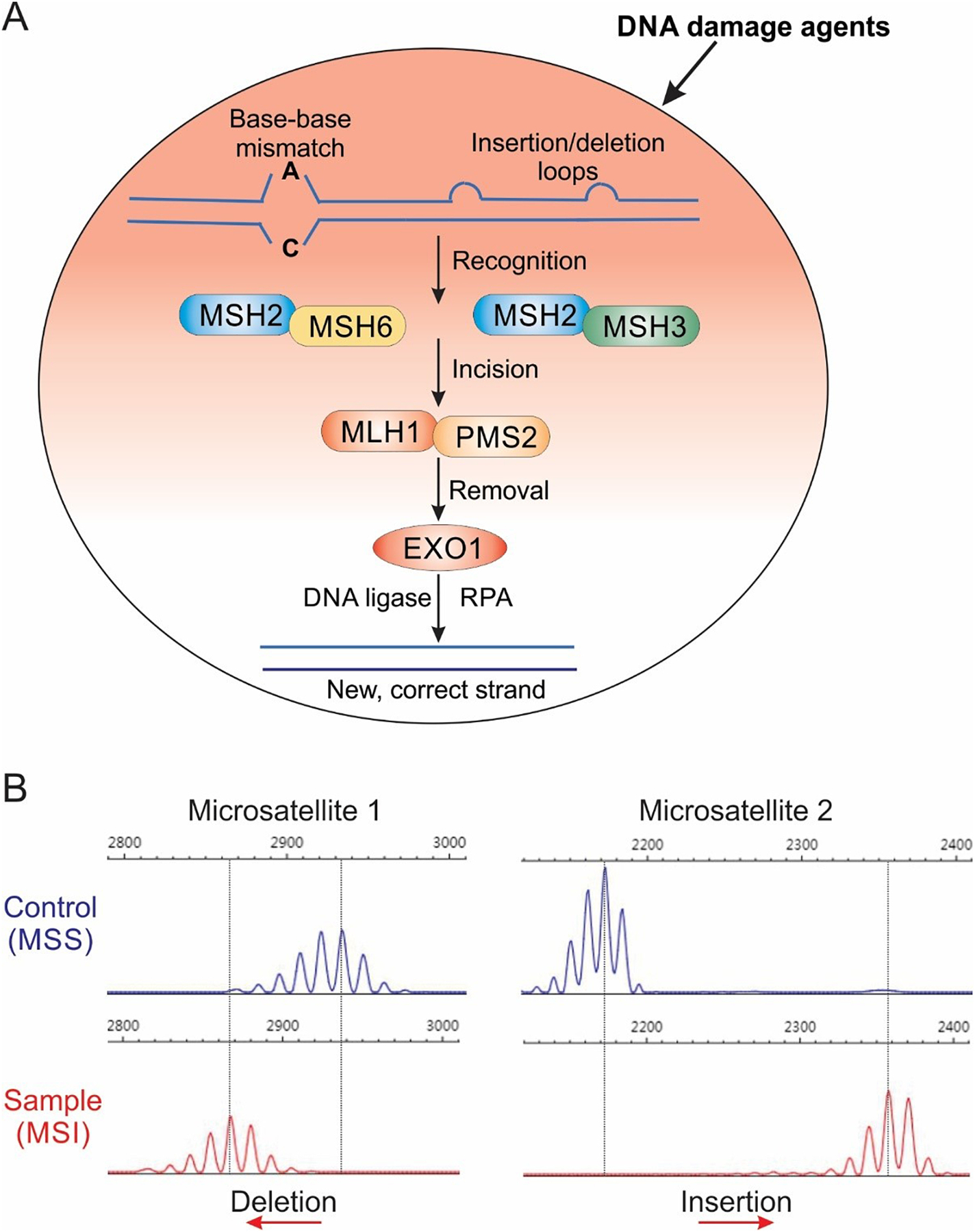
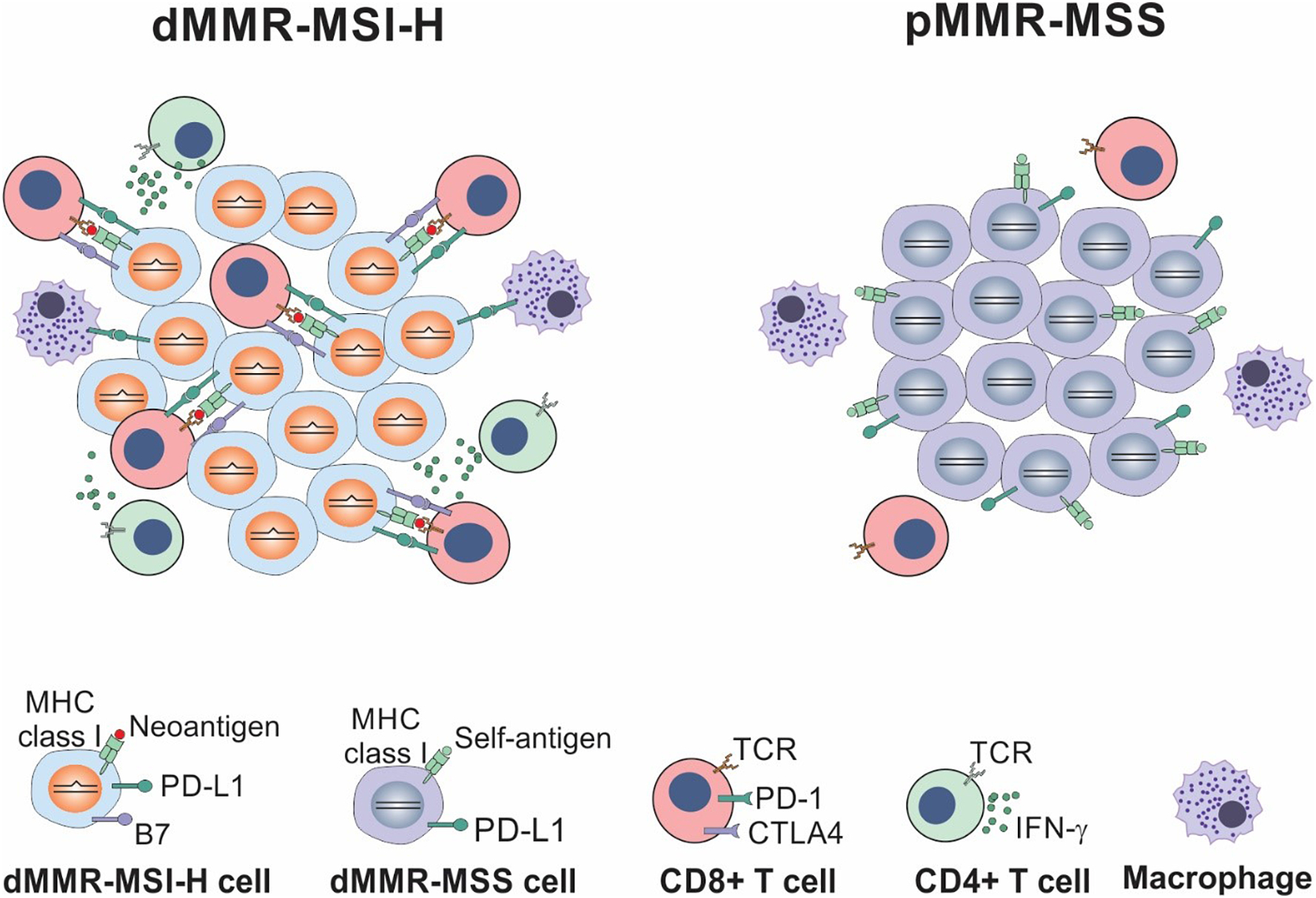
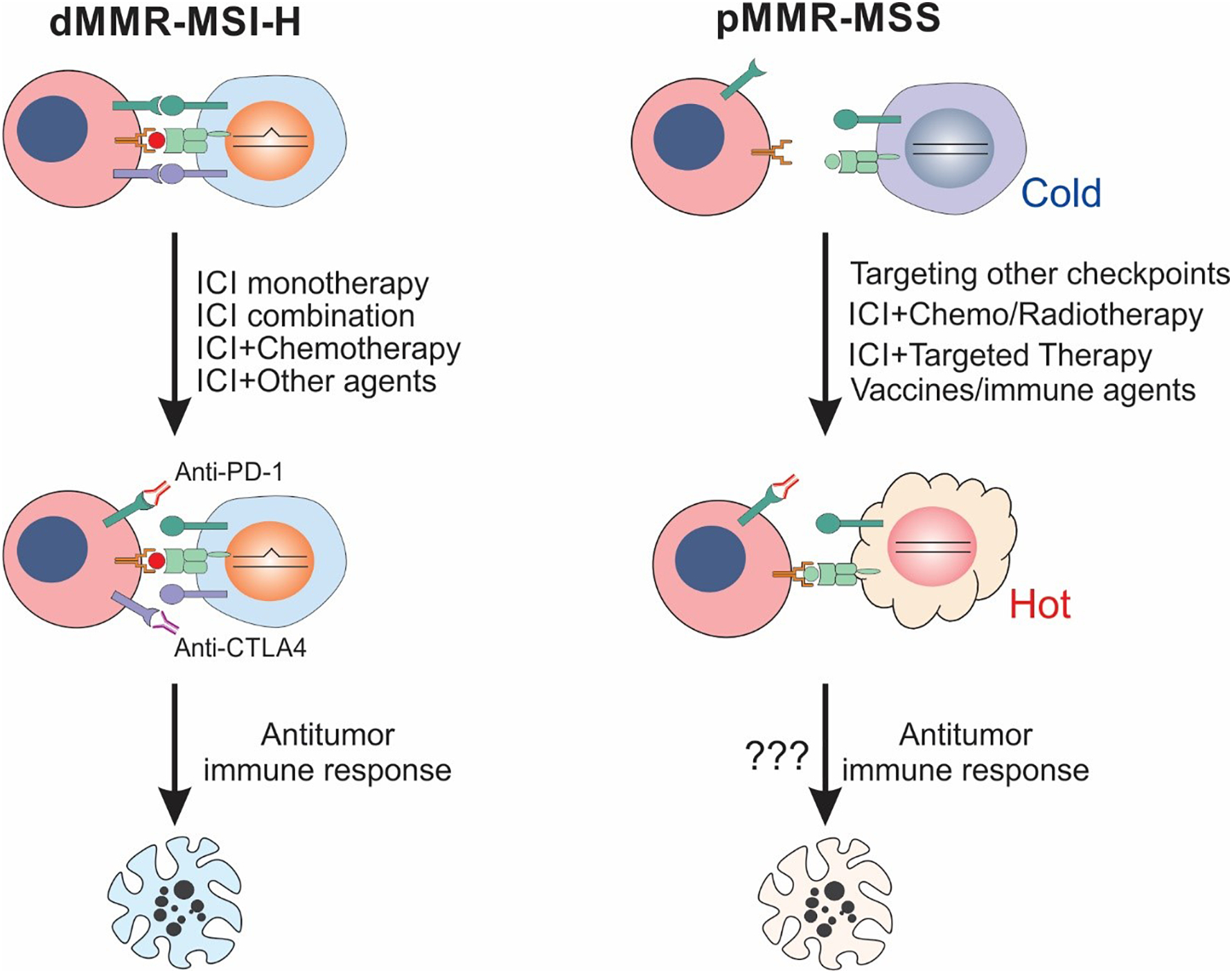
Colorectal cancers (CRCs) with deficient mismatch repair (dMMR) or microsatellite instability-high (MSI-H) often have sustained responses to immune checkpoint inhibitors (ICIs) including selective monoclonal antibodies against Program Death 1 (PD-1), Programmed Death Ligand 1(PD-L1), and cytotoxic T lymphocyte associated antigen 4 (CTLA-4). However, a substantial fraction of dMMR CRCs do not respond or ultimately develop resistance to immunotherapy. The majority (~85%) of CRCs are MMR proficient (pMMR) or microsatellite stable (MSS) and lack response to ICIs. Understanding the biology and mechanisms underlying dMMR-associated immunogenicity is urgently needed for improving the therapeutic efficacy of immunotherapy on CRC. Compared to pMMR/MSS CRCs, dMMR/MSI CRCs typically have increased tumor mutational burden (TMB), lower response rate to 5-fluorouracil-based chemotherapy, distinctive immunological features such as high tumor-infiltrating lymphocytes (TILs), and better prognosis. Here, we review the current understanding of the clinical relevance of dMMR/MSI in CRCs, the molecular basis and rationales for targeting dMMR CRC with immunotherapy, and clinical approaches using ICIs as single agents or in combination with other therapies for MSI-H CRCs. Furthermore, we address the potential strategies to sensitize pMMR/MSS CRC to immunotherapy by converting an immunologically "cold" microenvironment into a "hot" one.
Keywords: Colorectal cancer; Combination therapy; Immune checkpoint inhibitors; Immunotherapy; Microsatellite instability; Mismatch repair deficiency.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- Siegel RL, Miller KD, Jemal A, Cancer statistics, 2019, CA Cancer J Clin 69 (2019) 7–34. - PubMed
-
- Chu E, An update on the current and emerging targeted agents in metastatic colorectal cancer, Clinical colorectal cancer 11 (2012) 1–13. - PubMed
-
- Schachter J, Ribas A, Long GV, et al. , Pembrolizumab versus ipilimumab for advanced melanoma: final overall survival results of a multicentre, randomised, open-label phase 3 study (KEYNOTE-006), Lancet 390 (2017) 1853–1862. - PubMed
-
- Eggermont AMM, Blank CU, Mandala M, et al. , Adjuvant Pembrolizumab versus Placebo in Resected Stage III Melanoma, N Engl J Med 378 (2018) 1789–1801. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
