

The early impact of COVID-19 on mental health and community physical health services and their patients' mortality in Cambridgeshire and Peterborough, UK
- PMID: 33035957
- PMCID: PMC7508053
- DOI: 10.1016/j.jpsychires.2020.09.020
The early impact of COVID-19 on mental health and community physical health services and their patients' mortality in Cambridgeshire and Peterborough, UK
Abstract
Background: COVID-19 has affected social interaction and healthcare worldwide.
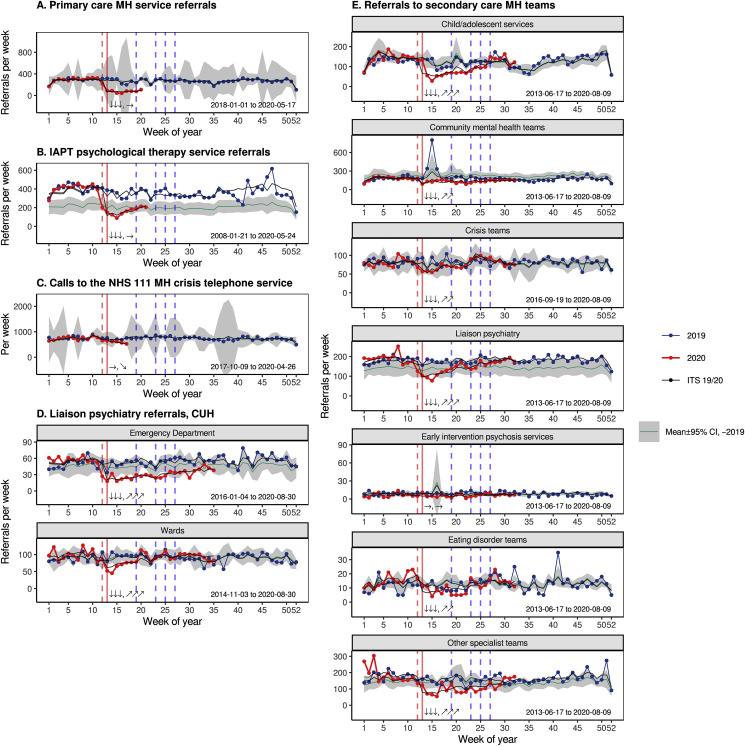
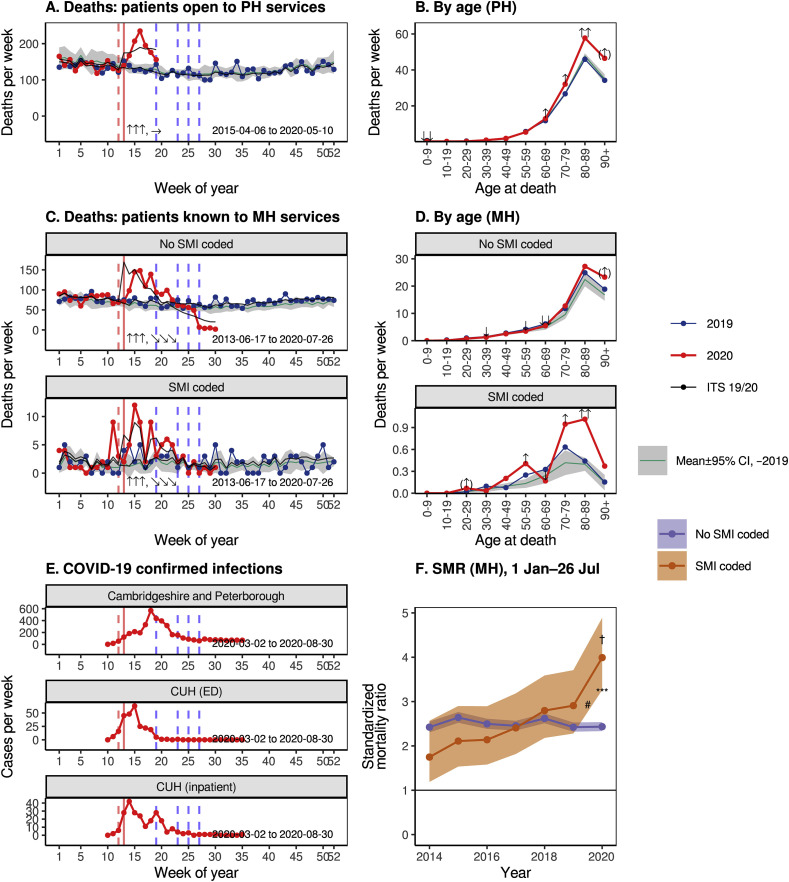
Methods: We examined changes in presentations and referrals to the primary provider of mental health and community health services in Cambridgeshire and Peterborough, UK (population ~0·86 million), plus service activity and deaths. We conducted interrupted time series analyses with respect to the time of UK "lockdown", which was shortly before the peak of COVID-19 infections in this area. We examined changes in standardized mortality ratio for those with and without severe mental illness (SMI).
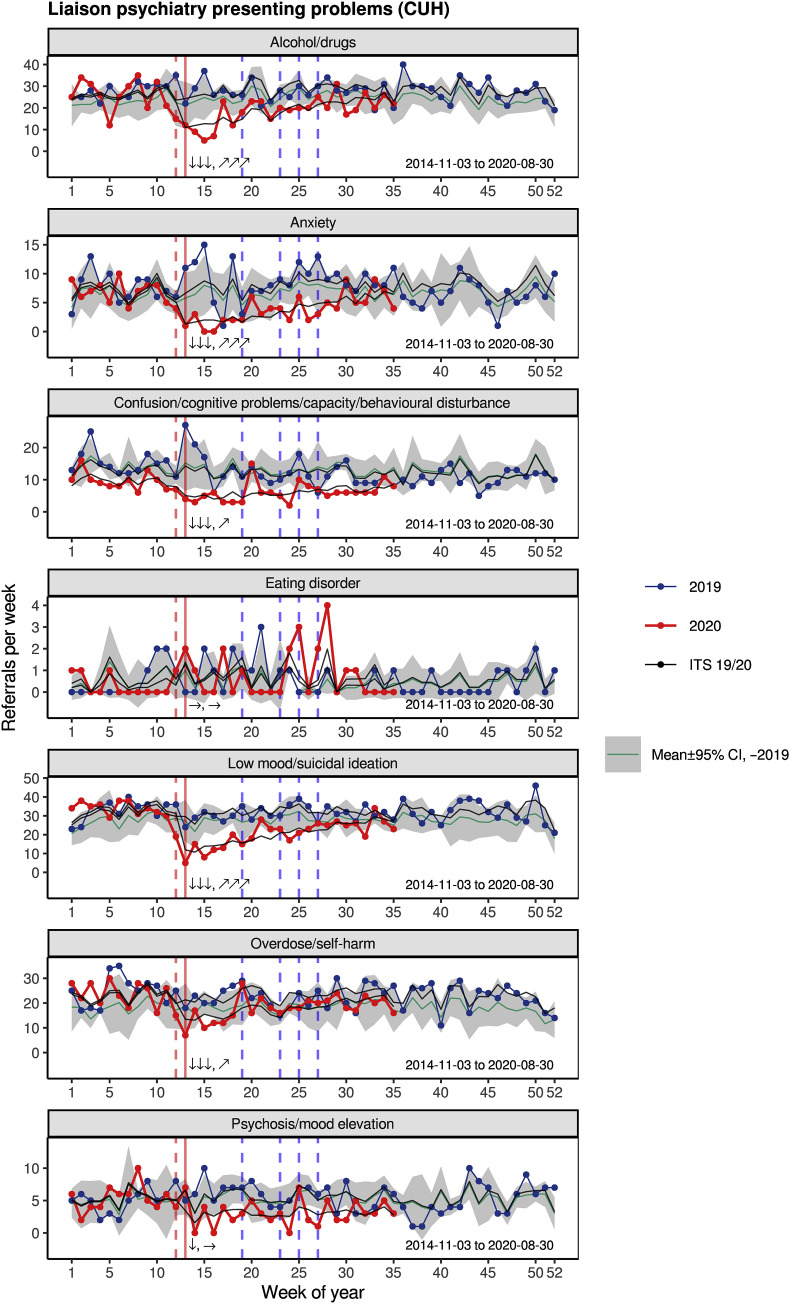
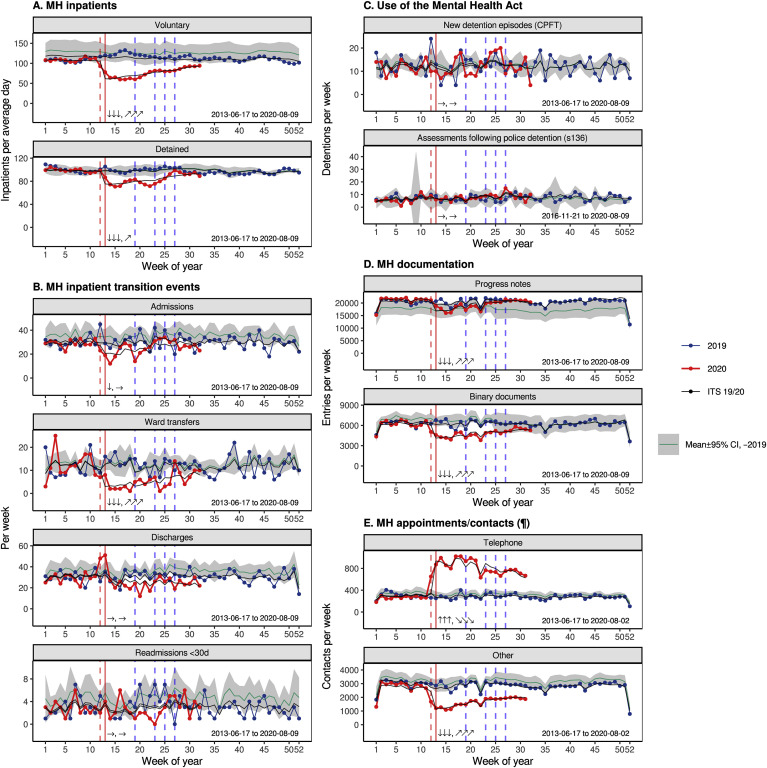
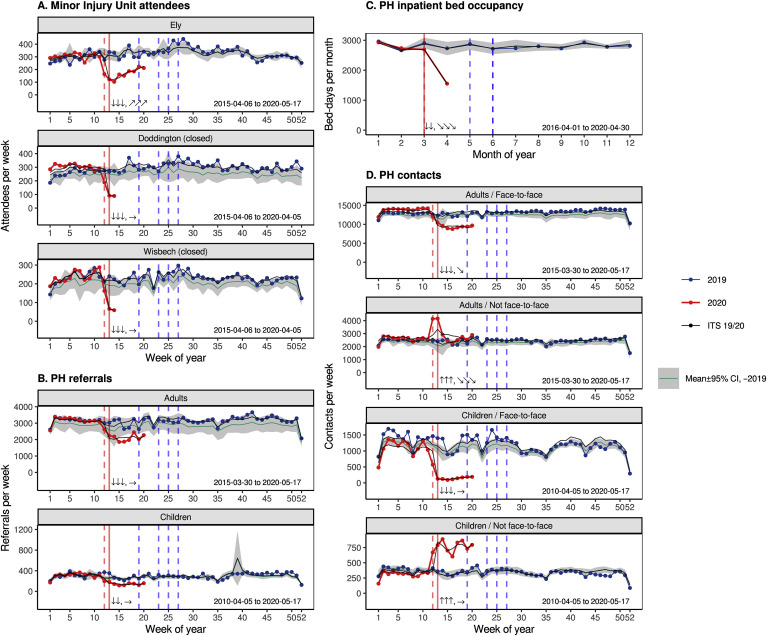
Results: Referrals and presentations to nearly all mental and physical health services dropped at lockdown, with evidence for changes in both supply (service provision) and demand (help-seeking). This was followed by an increase in demand for some services. This pattern was seen for all major forms of presentation to liaison psychiatry services, except for eating disorders, for which there was no evidence of change. Inpatient numbers fell, but new detentions under the Mental Health Act were unchanged. Many services shifted from face-to-face to remote contacts. Excess mortality was primarily in the over-70s. There was a much greater increase in mortality for patients with SMI, which was not explained by ethnicity.
Conclusions: COVID-19 has been associated with a system-wide drop in the use of mental health services, with some subsequent return in activity. "Supply" changes may have reduced access to mental health services for some. "Demand" changes may reflect a genuine reduction of need or a lack of help-seeking with pent-up demand. There has been a disproportionate increase in death among those with SMI during the pandemic.
Keywords: Alcohol and substance misuse; Anxiety; COVID-19/SARS-CoV-2 coronavirus pandemic; Depression; Mortality; Self-harm; Severe mental illness (SMI); Suicidality.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
- •
Several authors (PBJ, BRU, AM, ETB, ESO, JBD, CFH, FJT, RNC) are CPFT clinicians involved in delivering some of the services discussed here and two (BRU, FJT) are clinical directors and therefore involved in managing them.
- •
PBJ is a scientific advisory board member for Janssen and Recordati.
- •
BRU is clinical director of the Windsor Unit at Fulbourn Hospital (CPFT), which delivers clinical trials in dementia/mild cognitive impairment for academic and commercial organisations without personal benefit, and is the clinical lead for dementia for the NIHR Clinical Research Network (CRN) in the East of England. His salary is part-funded by the NIHR CRN. He has been principal investigator on trials for Axovant, Lilly, and EIP Pharma; his institution has benefited from payment for research carried out but he has not personally received any money. His wife is the lead for mental health for Suffolk Clinical Commissioning Group.
- •
AM’s salary is part-funded by the Anna Freud National Centre for Children and Families, a mental health charity.
- •
ETB is a scientific advisory board member for Sosei Hepares, and was a half-time employee of GlaxoSmithKline until May 2019.
- •
RNC consults for Campden Instruments Ltd and receives royalties from Cambridge University Press, Cambridge Enterprise, and Routledge.
- •
SC, SB, EFO, JBD, CFH, FJT, JDA, MPS, and JRL have nothing else to disclose.
Figures
References
-
- Banks J., Xu X. 2020. The mental health effects of the first two months of lockdown and social distancing during the Covid-19 pandemic in the UK. Published online June 10. - DOI
-
- Dalgaard P. Second ed. Springer; 2008. Introductory Statistics with R.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
