

High mortality among hospital-acquired COVID-19 infection in patients with cancer: A multicentre observational cohort study
- PMID: 33035991
- PMCID: PMC7470707
- DOI: 10.1016/j.ejca.2020.08.017
High mortality among hospital-acquired COVID-19 infection in patients with cancer: A multicentre observational cohort study
Abstract
Introduction: Studies suggest that patients with cancer are more likely to experience severe outcomes from COVID-19. Therefore, cancer centres have undertaken efforts to care for patients with cancer in COVID-free units. Nevertheless, the frequency and relevance of nosocomial transmission of COVID-19 in patients with cancer remain unknown. The goal of this study was to determine the incidence and impact of hospital-acquired COVID-19 in this population and identify predictive factors for COVID-19 severity in patients with cancer.
Methods: Patients with cancer and a laboratory-confirmed diagnosis of COVID-19 were prospectively identified using provincial registries and hospital databases between March 3rd and May 23rd, 2020 in the provinces of Quebec and British Columbia in Canada. Patient's baseline characteristics including age, sex, comorbidities, cancer type and type of anticancer treatment were collected. The exposure of interest was incidence of hospital-acquired infection defined by diagnosis of SARS-CoV-2 ≥ 5 days after hospital admission for COVID-unrelated cause. Co-primary outcomes were death or composite outcomes of severe illness from COVID-19 such as hospitalisation, supplemental oxygen, intensive-care unit (ICU) admission and/or mechanical ventilation.
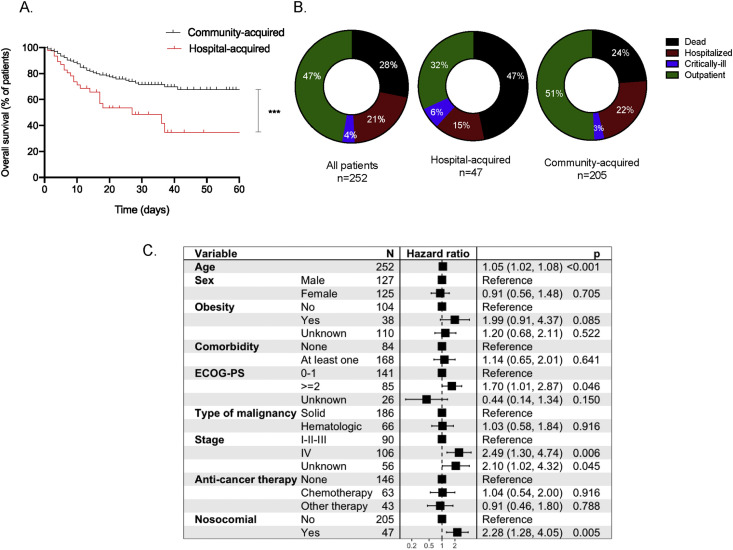
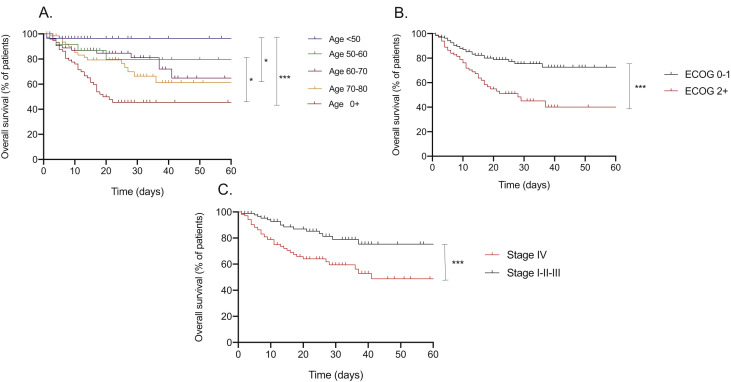
Results: A total of 252 patients (N = 249 adult and N = 3 paediatric) with COVID-19 and cancer were identified, and the majority were residents of Quebec (N = 233). One hundred and six patients (42.1%) received active anticancer treatment in the last 3 months before COVID-19 diagnosis. During a median follow-up of 25 days, 33 (13.1%) required admission to the ICU, and 71 (28.2%) died. Forty-seven (19.1%) had a diagnosis of hospital-acquired COVID-19. Median overall survival was shorter in those with hospital-acquired infection than that in a contemporary community-acquired population (27 days versus unreached, hazard ratio (HR) = 2.3, 95% CI: 1.2-4.4, p = 0.0006. Multivariate analysis demonstrated that hospital-acquired COVID-19, age, Eastern Cooperative Oncology Group status and advanced stage of cancer were independently associated with death.
Interpretation: Our study demonstrates a high rate of nosocomial transmission of COVID-19, associated with increased mortality in both univariate and multivariate analysis in the cancer population, reinforcing the importance of treating patients with cancer in COVID-free units. We also validated that age and advanced cancer were negative predictive factors for COVID-19 severity in patients with cancer.
Keywords: COVID-19; Cancer; Hospital-acquired; Nosocomial.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement BR and AE declare grant support from Astra Zeneca (grant number: N/A). Other authors have no conflict of interest to declare.
Figures
Comment in
-
Prevention of healthcare-associated respiratory-viral infections amongst oncology inpatients: Infection prevention outcomes during coronavirus disease-2019 pandemic.Eur J Cancer. 2021 Apr;147:117-119. doi: 10.1016/j.ejca.2021.01.017. Epub 2021 Jan 21. Eur J Cancer. 2021. PMID: 33640740 Free PMC article. No abstract available.
References
-
- WHO) WHO Coronavirus situation report. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio...
-
- Center JHUaMCR COVID-19 dashboard by the center for systems science and engineering (CSSE) at johns hopkins university (JHU) https://coronavirus.jhu.edu/map.html
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
