

Variation in surgical demand and time to hip fracture repair: a Canadian database study
- PMID: 33036609
- PMCID: PMC7547438
- DOI: 10.1186/s12913-020-05791-5
Variation in surgical demand and time to hip fracture repair: a Canadian database study
Abstract
Background: Competing demands for operative resources may affect time to hip fracture surgery. We sought to determine the time to hip fracture surgery by variation in demand in Canadian hospitals.
Methods: We obtained discharge abstracts of 151,952 patients aged 65 years or older who underwent surgery for a hip fracture between January, 2004 and December, 2012 in nine Canadian provinces. We compared median time to surgery (in days) when demand could be met within a two-day benchmark and when demand required more days, i.e. clearance time, to provide surgery, overall and stratified by presence of medical reasons for delay.
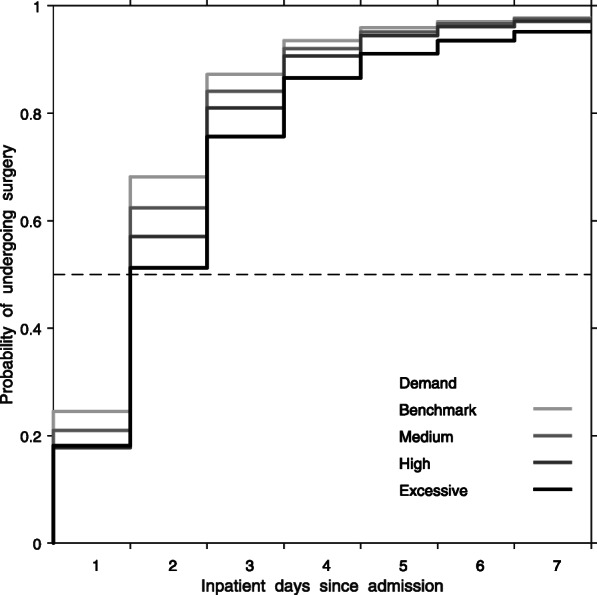
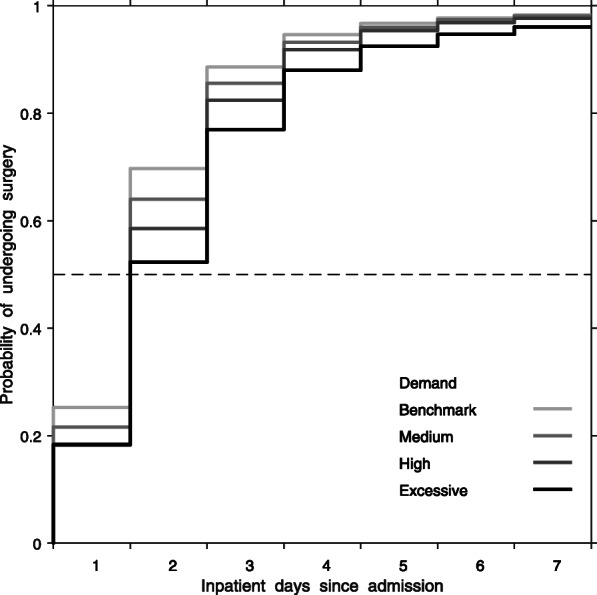
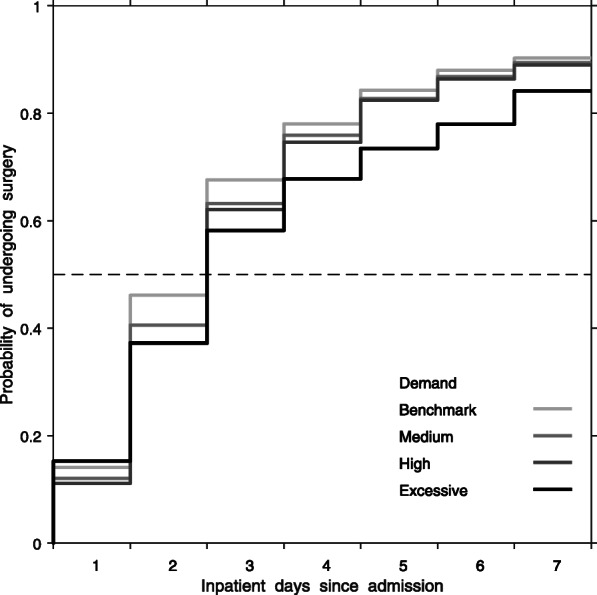
Results: For persons admitted when demand corresponded to a 2-day clearance time, 68% of patients underwent surgery within the 2-day benchmark. When demand corresponded to a clearance time of one week, 51% of patients underwent surgery within 2 days. Compared to demand that could be served within the two-day benchmark, adjusted median time to surgery was 5.1% (95% confidence interval [CI] 4.1-6.1), 12.2% (95% CI 10.3-14.2), and 22.0% (95% CI 17.7-26.2) longer, when demand required 4, 6, and 7 or more days to clear the backlog, respectively. After adjustment, delays in median time to surgery were similar for those with and without medical reasons for delay.
Conclusion: Increases in demand for operative resources were associated with dose-response increases in the time needed for half of hip fracture patients to undergo surgery. Such delays may be mitigated through better anticipation of day-to-day supply and demand and increased response capability.
Keywords: Demand; Hip fracture; Surgical delay; Time to surgery; Variation.
Conflict of interest statement
The authors declare that (1) BS, PG and the Collaborative have received grants from the Canadian Institutes of Health Research related to this work. (2) PG also receives funding and fees from the British Columbia Specialists Services Committee for work around hip fracture care not related to this manuscript and from Stryker Orthopedics (as a product development consultant). He is a board member and shareholder in Traumis Surgical Systems Inc. and a board member for the Canadian Orthopedic Foundation. He also serves on the speakers’ bureaus of Stryker Canada. (3) SNM receives salary support from the Fonds de Recherche du Québec en Santé and reports research grants from Amgen Canada, and from Merck. (4) KS has received funding from the National Institute of Health Research, the Chartered Society of Physiotherapy UK, and UK Research and Innovation for work around hip fracture care not related to this manuscript. (5) LB receives salary support as the Dr. David Magee Endowed Chair for Musculoskeletal Research from the Faculty of Rehabilitation Medicine at the University of Alberta. (6) JMS is a Scholar of the Michael Smith Foundation for Health Research (MSFHR). (7) JDK, LK, ARL, EJH declare they have no conflicts of interests.
Figures
References
-
- Institute of Medicine (1993) Committee on monitoring access to personal health care services. Access to health care in America. National Academy Press, Washington, DC. ttps://archive.ahrq.gov/research/findings/nhqrdr/nhdr11/chap9.html [Accessed on August 21, 2019].
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
